Download
1 / 142
1.42k likes | 1.42k Views
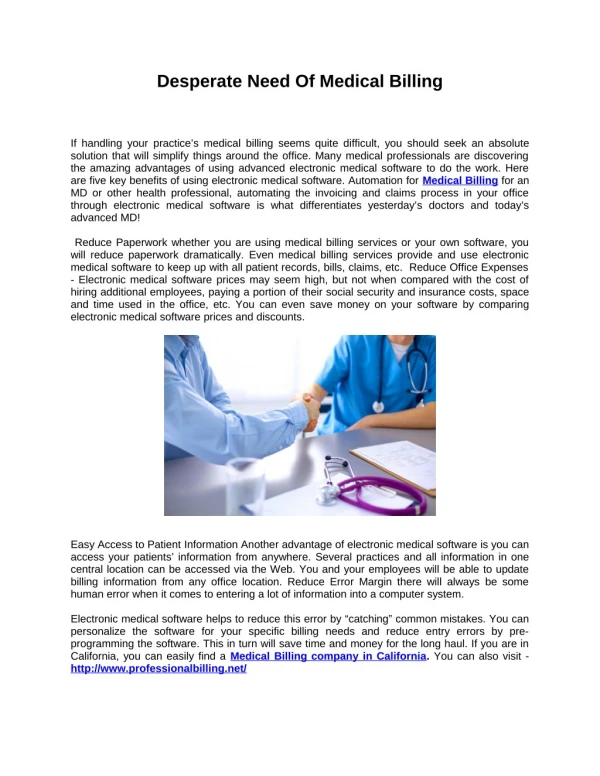
This case study explores the presentation and management of a young patient who presented with fever and seizure. The importance of early intervention and appropriate treatment in cases of status epilepticus is discussed.

E N D
Desperate Maladies, Desperate Remedies Au Shek Yin QEH ICU Interhospital Grand Round 19/7/2011
Presented with fever and seizure • 18M • Student in PolyUniversity • Good past health • No family history of epilepsy • No history of drug abuse • TOCC –ve apart from mosquito bites at home
Collateral history • No rash in patient / family members / classmates • No retroocular pain • No parotitis/ testicular pain/ abdominal pain • No ear pain/ facial pain/ purulent ear/ nasal discharge/ No dental caries • No previous complaints of strange smells • No recent vaccination
On 14/5/2011 • Presented with high fever and generalized malaise 5 days before admission • Attended AED of hospital A on 14/5/2011 with sore throat, cough, running nose and nausea • Given ampicillin, paracetamol and discharged home
On 19/5/2011 • Patient subjectively felt better. He attended a meeting with his classmates on 19/5/2011 since 7pm • Tired looking throughout the meeting and was found collapse with facial twitching at 10pm • GCS 8/15 when attended QEH AED • Intubated at AED for airway protection • Still noted facial twitching
Urine for toxicology kit and ketamine –ve • Urgent CT brain done and direct admission to ICU
Arrived at ICU at 00:10 • Intubated, GCS E1M1VT • Afebrile • BP 100/46 pulse 100 Hstix 8 • No rash / No needle marks • No LN • Neck soft • Pupil 4-5mm equal with sluggish response • 4 limb flaccid on arrival • Repeated attacks of GTCs
Initial investigations • ECG sinus HR 100 with normal QT and QRS • Blood test taken at AED • WBC 8.2 plt 155 • INR 1.01 APTT 34.5 • ABG: pH 7.18 PCO2 6.3 PO2 72.7 BE -11 • Blood for electrolytes unremarkable
Boluses of dormicum and propofol given and started dormicum infusion • phenytoin was given with loading and maintenance • Needed to start noradrenaline to maintain BP • Clinical seizure only transiently aborted • Toxicology saved and proceeded to LP
LP • OP 13cm CSF • Clear CSF • Started empirical acyclovir, rocephin, penicillin G • Later pen G shifted to ampicillin for better listeria monocytogenes cover • Added IVIG for possible EV71 and enterovirus rhomboencephalitis • Also added tamiflu for possible influenza encephalitis
Still repeated seizure attacks 20min after admission at 00:30 • Recurrent seizure again • in less than 10 min with boluses of propofol, dormicum, dilantin and on dormicum infusion were given
History The earliest description of SE is between 718-61 BC during Neo-Babylonian era. Clark and Prout described the natural course of SE in 38 patients unaffected by anti-convulsants. Clark LP, Prout TP. Status epilepticus: a clinical and pathological study in epilepsy. Am J Insanity 1903;60:291-306, 60:645-75, 61:81-108.
Classification • Gastaut: there are as many types of status as there are types of epileptic seizures • The term status is used “when a seizure persists for a sufficient time and is repeated frequently enough to produce a fixed or enduring epileptic condition” Gastaut H. Classification of status epilepticus. Adv Neurol 1983;3415-35.
A definition is needed :30min • More than 40% of seizures lasting from 10-29 min stops spontaneously without treatment • Mortality of seizures from 10-29 min vs seizures more than 30 min 2.6% versus 19% (p<0.001) DeLorenzo RJ, Hauser WA, Towne AR, and et al. A prospective, population-based epidemiologic study of status epilepticus in Richmond, Virginia. Neurology 1996;46:1029-1035.
Strong statistical reasons for using 5 min as time limit criterion • Mean duration of generalized convulsive seizures in adults ranges from 52.9 sec to 62.2 sec (with SD 14). None of these seizures exceed 2 min. • Wasterlain CG. Definition and classification of status epilepticus. The international meeting on status epilepticus, Santa Monica, CA; 1997(Abstract) • Lowenstein DH. Bleck T, Macdonald RL. It’s time to revise the definition of status epilepticus. Epilepsia 1999;40:164-169. • Meldrum BS. The revised operational definition of generalized tonic-clonic status epilepticus in adults. Epilepsia 1999;40:123-124. • Shorvon S. The management of status epilepticus. J Neurol Neurosurg Psychiatry 2001;70 (suppl 2):1122-1127.
Reasons for 5 min as the time limit • With 5 min, there will be 18-20 standard deviations away from the norm. This indicates that SE is something distinct and unusual. This definition will unlikely generate confusion or delay in treatment • Theodore WH, Porter RJ, Albert P and et al. The secondarily generalized tonic-clonic seizure: a videotape analysis. Neurology 1994;44:1403-1407. • Kramer R, Levisohn P. The duration of secondarily generalized tonic-clonic seizures. Epilepsia 1992;33:68 (abstract)
3 cellular mechanisms of SE • Membrane instability: Further classified to increase excitability (pentylenetetrazol model), or decrease inhibitory influences (picrotoxin model) the latter more common • Post-synaptic receptor alterations:Either increase in stimulation of excitatory receptors or decrease inhibitory receptors • Neurotransmitter:Excitatory transmitter may cause seizure upon release, and absence of inhibitory transmitters, e.g.γaminobutyric acid or GABA may lead to seizure activities • Michael J. Neurolgic intensive care: status epilepticus. Crit Care Med 1993 Sep (Supl);21:9: S335-S336. • Drislane FW. Evidence against permanent neurologic damage from nonconvulsive status epilepticus. J Clin Neurophysiol 1999;16:323-331. • Kaplan PW. Prognosis in non-convulsive status epilepticus. Epileptic Disorder 2000;2:185-193.
Brain injury • Cell damage due to excessive excitatory neurotransmitter release, which activates N-methyl-D-asparate receptors and voltage-activated calcium channels, allowing calcium to enter into the cells. • Lipton SA, Rosenberg PA. Excitatory amino acids as final common pathway for neurologic disorders. N Eng J Med 1994;330:63-22.
A high Ca concentration leads to generation of reactive oxygen species via activation of nitric oxide synthase, uncouples oxidative phosphorylation in mitochondria and activates lipase, protease, endonuclease and many others catabolic enzymes that adversely affect cell function. • Holmes GL, Ben-Ari Y. The neurobiology and consequences of epilepsy in the developing brain. Pediatr Res 2001;49:320-25.
Self perpetuating nature of SE • First recognized in 19th century by Trousseau. • Well demonstrated in animal models • Initial SE can be easily blocked by drugs • However once established, it will be perpetuated. • SE causes neuronal damage from ongoing electographic activities, particularly in hippocampus, leading to excessive activation of glutamate receptors
Pathophysiology of self-sustaining status epilepticus • a speculative mechanism with three phases • First phase (between a few seconds to a few minutes): • Existing receptors move from the synaptic membrane into the endosomes, or be mobilized from storage sites to the synaptic membrane, hence drastically change the excitability by altering the number of inhibitory and excitatory receptors in the synaptic cleft.
Neuropeptides change • Second phase (between minutes to hours): • There are plastic changes in neuropeptide modulators, with increase expression of proconvulsive neuropeptides and depletion of inhibitory neuropeptides, hence contributing to a state of raised excitability. • Liu H, Mazarati AM, Katsumori H, Sanker R, Wasterlein CG. Substance P is expressed in hippocampal principal neurons during status epilepticus and plays a critical role in the maintenance of status epilepticus. Proc Natl Acad Sci USA 1999;96:5286-91. • Vezzani A, Sperk G, Colmers WF. Neuropeptide Y: emerging evidence for a functional role in seizure modulaton. Trends Neurosci 1999;22:25-30.
Gene expression change • Final phase (hours, days and more): • Long term change in gene expression. The change in gene expression is a result of seizure-induced neuronal death and neuronal reorganization, with plastic adaptation to seizure activity • Wasterlein CG. Inhibition of cerebral protein synthesis by epileptic seizures without motor manifestations. Neurology 1974;24:175-80.
Back to Our patient It is now 30 min after admission to ICU • SE not controlled • We have already given boluses of dormicum, propofol, phenytoin and put on dormicum infusion
Added regular sodium valproate (Epilim) and phenobarbitone (Luminal) • Seizure still not yet aborted!
It was then 01:00, about 50 min after ICU admission What could be done further?
Started thiopentone with loading and infusion and stopped dormicum and propofol after thiopentone infusion ( I hoped … ) • Seizure finally aborted…
Recurrent seizure again at around 01:30, ~ 1 hr 20 min after ICU admission
Thiopentone stepped up to 12ml/ hr ( ~ 5mg/kg/ hr ) • Resumed propofol and dormicum infusion • Also started clobazem • Seizure finally aborted
Where to stop ? When to stop ? • Controversy about whether both clinical and EEG seizures should be completely controlled • Many use burst-suppressionon EEG and aim for complete control of both, whereas some aim for control of clinical seizures (without EEG monitoring). • Bleck TP. Management approaches to prolonged seizures and status epilepticus. Epilepsia 1999;(40 Suppl 1):S59-S63. • Bleck TP. Refractory status epilepticus in 2001. Arch Neurol 2002;59:188-189.
In a survey, 56% aimed at burst-suppression while 41% titrated for seizure elimination. Claassen J, Hirsch LJ, Mayer SA. Treatment of status epilepticus: a survey of neurologists. J Neurol Sci 2003;211:37-41. • But even with burst suppression, the degree of suppression is unclear. Some used a burst-suppression pattern as endpoint, aiming for inter-burst interval of at least 5 seconds in duration. • Sahin M, Menache C, Holmes GL and et al. Outcome of severe refractory status epilepticus in children. Epilepsia 2001:42: 1461-67. • Sahin M, Riviello JJ. Prolonged treatment of refractory status epilepticus in a child. J Child Neurol 2001;16:147-150.
Persistent seizure control is better with electrocerebral inactivity on EEG (17/20) than burst suppression pattern (6/12). • Krishnamurthy KB, Drislane FW. Relapse and survival after barbiturate anaesthetic treatment of refractory status epilepticus. Epilepsia 1996;37:863-867.
However hypotension often occurs when titration for electrocerebral inactivity. • Claassen J, Hirsch LJ, Emerson RG and et al. Treatment of refractory status epilepticus with pentobarbital, propofol, or midazolam: a systematic review. Epilepsia 2002;43:146-153.
High dose suppression therapy • HDST usually for 12 to 24 hours, and then tapered the infusion. If SE recurs, HDST can be started • Prolonged HDST considered if potential good prognosis: healthy patient before the SE, self-limiting disease, no disease in work up including neuroimaging study. • Mirski MA, Williams MA, Hanley DF. Prolonged pentobarbital and Phenobarbital coma for refractory generalized status epilepticus. Crit Care Med 1995;23:400-404.
However in one study, 7 out of 22 (32%) returned to baseline. But all 7 subsequently developed refractory epilepsy: epilepsy recurrence upon tapering, within 1 to 16 months. • Hence prognosis must be taken into account when using such extreme therapy. • Sahin M, Menache CC, Holmes GL. Outcome of acute symptomatic refractory status epilepticus in children. Neurology 2003;61:398-401.
Double-blind Randomized Comparison of 4 i.v. Treatments in Overt of Generalized Convulsive Status (n=384)
Stage 1Premonitory/Early Status (0-30/60 minutes) • Benzodiazepines drugs of choice: Lorazepam, 4 mg iv, may be repeated after 10 min Diazepam, 10-20 mg iv (5 mg/min), may be repeated after 10 minutes midazolam, clonazepam • Out-of-hospital therapy Rectal diazepam Buccal/intranasal/im midazolam
Benzodiazepine- the drug of choice • Class 1 evidence • Although IV lorazepamand diazepam have similar complicationrates, lorazepam is the preferredtherapy because of efficacy. • Although diazepamrapidly enters the brain becauseof its high-lipid solubility, itsclinical effect is diminished by its rapidsystemic distribution. Lorazepam has alonger duration of action and a lowerrisk of seizure recurrence.
The Veterans Affairs Status EpilepticusCooperative Study Group report: at least one-third ofthe time, initial benzo fails to stopSE. And a second medicationis usually also unsuccessful • Nevertheless,American and European protocolscall for a second treatment, anonbenzodiazepine, to be given for persistentSE. The most commonly usedoptions are fosphenytoin or phenytoin.
Stage 2Established Status Epilepticus • Conventional treatment: Phenytoin/fosphenytoin iv at 50 mg/min Fosphenytoin iv at 150 mg of phenytoin equivalents /min Phenobarbitone, 10mg/kg iv at 100 mg/min • Alternatives: Valproate, levetiracetam, benzodiazepine infusion Courtesy of T. Tomson, 2010






![[PDF] Desperate Measures By Stuart Woods Free Download](https://cdn4.slideserve.com/8047900/pdf-desperate-measures-by-stuart-woods-free-dt.jpg)

