Download
1 / 58
590 likes | 1.9k Views
腹 部 The Abdomen. 第一节 腹部体表标志及分区 The landmarks of the anterior abdominal wall and segments dividing. 腹部范围 体表标志 肋弓下缘、 胸骨剑突、髂 嵴、 髂前上 嵴、脐、腹直 肌外缘、腹中 线、腹股沟韧 带、第 12 肋骨 等。. 腹部分区 临床常用九区法和四区法。. 第二节 视 诊 Inspection of the abdomen. 腹部视诊的方法 腹部视诊的主要内容 (一)腹部外形 健康成人腹部外观对称、腹部平坦

E N D
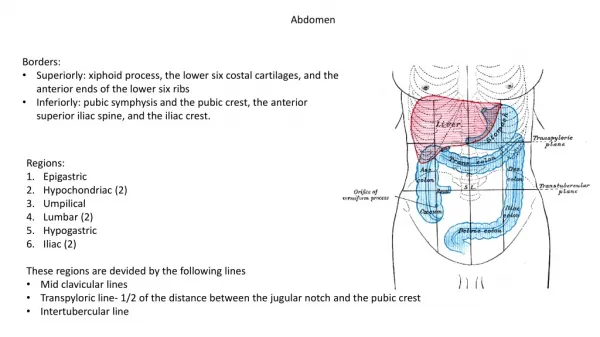
第一节 腹部体表标志及分区The landmarks of the anterior abdominal wall and segments dividing
腹部范围 • 体表标志 肋弓下缘、 胸骨剑突、髂 嵴、 髂前上 嵴、脐、腹直 肌外缘、腹中 线、腹股沟韧 带、第12肋骨 等。
腹部视诊的方法 • 腹部视诊的主要内容 (一)腹部外形 健康成人腹部外观对称、腹部平坦 (二)呼吸运动 (三)腹壁静脉 (四)蠕动波 胃蠕动波——幽门和肠梗阻; 肠蠕动波——肠梗阻 (五)腹壁其它情况
第三节 触 诊 Palpation of the abdomen
触诊内容 (一)腹壁紧张度 腹壁紧张度增加 板状腹(急性腹膜炎), 揉面感(结核性腹膜炎、癌性腹膜炎); 局部腹壁紧张(局部脏器炎症)。 腹壁紧张度减低或消失
触诊内容 (二)压痛及反跳痛 • 压痛常见原因: • 反跳痛原因: • 特定压痛点: 胆囊压痛点、麦氏点。
Localisation of foregut、 midgut and hindgut pain Foregut pain localises to epigastric area Midgut pain localises to periumbilical area Hind-gut pain localises to suprapubic areas Perception of visceral pain is localised to the epigastric、umblilcal or suprapubic region according to the embryological origin of the diseased organ.
肝触诊 脾触诊 胆囊触诊 肾触诊 膀胱触诊 胰触诊 脏器触诊 Palpation of the organs
第四节 叩 诊 Percussion of the abdomen
一、腹部叩诊音the sound of percussion in the abdomen 腹部正常叩诊音 为鼓音,其内有脏器 的部位叩诊音为浊音。
二.肝及胆囊叩诊 percussion of liver and gallbladder Positioning of the hand when percussing for the lower border of the liver. Percussion of the upper border of the liver.
临床意义: • 正常 • 肝浊音界扩大 • 肝浊音界缩小 • 肝浊音界消失 • 肝浊音界上移 • 肝浊音界下移 Atrophy of the liver may be detected by percussing the lower border.The area of resonance will extend above the costal margin.
对胆囊大小的确诊无意义,叩击 痛提示为胆囊炎。 胆囊叩诊
★脾浊音区扩大:脾肿大。 ★脾浊音区缩小:左侧气胸、胃扩张、鼓肠。 (三)胃泡鼓音和脾叩诊 percussion of stomach and spleen Percuss for the enlarged organ in the ninth intercostalspace anterior to the anterioraxillary line.
叩诊方法及定义 意义:腹腔内游离腹水在1000ml以上。 (四)移动性浊音Shifting dullness of ascites To confirm the presence of ascites,roll the patient into the right lateral position because this causes fluid to settle in the dependent right flank,whereas gas-filled bowel floats above to fill the left flank.A shift in thepositions of dullness and tympany indicates ftee fluid.
When percussing for ascites,(a)beginin the midline with your finger parallel to the lateral wall of the abdomen and (b)continue to the left flank.A change in the percussion note indicates a gas-fluid interface.
腹水的鉴别 肠潴留(有肠梗阻症状), 巨大卵巢囊肿(位于中腹部,浊音区不移动、尺压试验阳性)。
(五)脊肋角叩痛方法 • 意义(肾炎、肾盂肾炎、肾结石、肾结核和肾周围炎) Assessing the punch tenderness over the renal angles.
(六)膀胱叩诊percussion of bladder 尿潴留时 在耻骨联合上 可叩出呈圆形 的浊音区。但 应与肿大的子 宫、卵巢肿瘤、 腹水相鉴别。 Percuss for the fundus of the bladder from the level of the umbilicus.
(一)肠鸣音 bowel sounds • 正常:4-5次/每分。 • 肠鸣音活跃 • 肠鸣音亢进 • 肠鸣音减弱 • 肠鸣音消失。
(二)血管杂音(动脉和静脉) Bruits in the aorta and the vein • 中腹部收缩期血管杂音(喷射) 腹主动脉瘤或腹主动脉狭窄。 • 左右上腹部收缩期血管杂音 肾动脉狭窄(年轻高血压)。 • 肝包块听到吹风样杂音 左叶肝癌 • 静脉性杂音:脐周或上腹部连续性嗡鸣样静脉杂音 门静脉高压侧枝循环形成
Position of the stethoscope when listening for bruits renal artery in(a) the aorta and (b) the.
position for a Position of the stethoscope when listening liver bruit.
(三)摩擦音 sound of rub 摩擦音—脾梗 塞、脾周围炎、肝 周围炎、胆囊炎累及局部腹膜。 Position of the stethoscope when listening for a splenic rub.
(四)搔弹音 • 肝下缘的测定, • 微量腹水(120ml)的测定.
第六节 腹部常见病的主要 症状和体征the main symptoms and signs of general abdominal diseases
一、胃、十二指肠溃疡peptic ucler • 腹痛特点 • .节律性: • .季节性: • .慢性反复发作 • 压痛点: • 胃溃疡; • 球部溃疡:
二、急性腹膜炎acute peritonitis • 急性弥漫腹膜炎 • 腹膜炎三联征阳性:腹壁肌紧张(板状腹)、腹部压痛、反跳痛。 • 其他:腹式呼吸消失或减弱,腹膨隆,移动性浊音(+),肝浊音界缩小或消失,肠鸣音减弱或消失。 • 局限性腹膜炎: • 症状和体征局限于病灶周围,也较急性弥漫腹膜炎轻。
三.肝硬化liver cirrosis • 症状: 消化不良症状+全身症状+肝功能不全症状 • 主要体征: • 面色灰暗、黄疸、蜘蛛痣、肝掌等。 • 肝脏:肿大 缩小,质地变硬,表面不光。 • 门脉高压的表现:腹水、静脉侧枝循环的建立和开放(三条)、脾肿大。
四、急性阑尾炎acute appendicitis • 症状: 转移性右下腹痛+恶心、呕吐、发烧等。 • 体征: • McBurney点(阑尾点)压痛和反跳痛 • 洛(Rovsing)氏征阳性 • 腰大肌征阳性(盲肠后位阑尾炎)
五、肠梗阻intestinal obstruction • 主要症状: 痛、吐、胀、闭。 • 主要体征: 急性病容、脱水征、休克表现;腹膨 隆,肠型及蠕 动波;腹壁紧张有压痛; 肠鸣音亢进(金属音调)。 麻痹性肠梗阻时肠鸣音减弱或消失。
六、腹部包块mass of abdomen 正常腹部可 触及的包块 On deep palpationof the abdomen,these structures may be felt.
六、腹部包块mass of abdomen 病理性(异常)包块 • 包块的描述: 位置、大小、形态、质地、压痛、 搏动、移动度。 • 包块常见的原因: 实质性脏器的病理肿大、空腔脏器 的扩张、炎性肿块肿瘤、寄生虫等。
第三节肛门与直肠 • 体位: • 1.肘膝位: • 2.左侧卧位: • 3。仰卧位或截石位: • 4.蹲位:用于检查直肠脱出、内痔及直肠息肉。 • 病灶位置描述方法:体位+钟表时针位。
一.视诊: • 观察肛门及周围粘膜颜色、皱折.肛门常见疾病:1.闭锁与狭窄2.肛门外伤与感染(肛门周围囊肿)3.肛裂、4.痔、(内痔、外痔、混合痔)、5.肛门直肠瘘、6.直肠脱垂。
二、触诊 • 体位、方法、用途 • 直肠常见病变: • A.剧烈触痛—肛裂、感染。 • B.柔软、光滑有弹性的包块—直肠息肉。 • C.坚硬凹凸不平的包块—直肠癌。 • D.黏液、脓液、血液—炎症、坏死组织(癌)。
一、脊柱弯曲度 • (一)生理性弯曲 • (二)病理性弯曲 ★脊柱后凸(kyphosis):多见于胸段。常见于佝偻病、结核病、强制性脊椎炎、脊椎退行性变、发育期姿势不良、脊椎骨软骨炎(Scheuerman)
★脊柱前凸(lordosis):多见于腰椎部位。常见于晚期妊娠、大量腹水、髋关节结核及先天性髋关节脱位。★脊柱侧凸:姿势性侧凸(posture scoliosis) ★器质性侧凸(organ scoliosis) • 病、慢性胸膜炎、胸膜粘连等。
二、脊柱活动度 • 正常活动度 • 活动受限:肌肉、肌韧带、椎间盘(关节)、椎骨破坏、外伤,临床常见颈椎、腰椎。