Download

1 / 30
300 likes | 532 Views
Overview. NHSC

E N D
1. Identifying and appraising new health technologies: the National Horizon Scanning Centre and the National Institute for Clinical Excellence James Raftery
Director, Health Economics Facility,
HSMC, University of Birmingham
2. Overview
3. Health Technology All interventions used to promote health, prevent and treat disease, and improve rehabilitation and long-term care.
Pharmaceuticals
Medical devices, biotechnology, biomaterials etc.
Diagnostic tests and procedures
Interventional procedures: surgery and radiological
Health promotion and screening programmes
Rehabilitation and other therapy
4. New and emerging health technologies Emerging - not yet adopted by a health care system:
Pharmaceuticals: phase ll or lll clinical trials or pre-launch
medical devices: prior to marketing, or within 6 months of marketing, or marketed but <10% diffused or localised to a few centres
New - in the phase of adoption, only available for clinical use for a short time, generally in the launch or early post-marketing stages.
5. Early warning systems in this context are stable units with reliable connections and sources that have several key features in common.
Early warning starts with some sort of horizon scanning � the systematic identification of emerging health technologies. Identification is followed by filtration and prioritisation to select those items most likely to warrant further assessment. Prioritisation is generally a circular process with information retrieval. Assessments, in our case a prediction of likely future impact, then need to be disseminated.
Early identification and assessment does not need to be undertaken by one organisation. Different parts of the process can be undertaken by different bodies.
Within England and Wales on a national basis the National Horizon Scanning Centre undertakes these process (explain which), producing a prediction of potential for impact, with the National Institute for Clinical Excellence (NICE) augmenting our assessment of potential for future impact, with a full assessment and appraisal of clinical and cost effectiveness. Early warning systems in this context are stable units with reliable connections and sources that have several key features in common.
Early warning starts with some sort of horizon scanning � the systematic identification of emerging health technologies. Identification is followed by filtration and prioritisation to select those items most likely to warrant further assessment. Prioritisation is generally a circular process with information retrieval. Assessments, in our case a prediction of likely future impact, then need to be disseminated.
Early identification and assessment does not need to be undertaken by one organisation. Different parts of the process can be undertaken by different bodies.
Within England and Wales on a national basis the National Horizon Scanning Centre undertakes these process (explain which), producing a prediction of potential for impact, with the National Institute for Clinical Excellence (NICE) augmenting our assessment of potential for future impact, with a full assessment and appraisal of clinical and cost effectiveness.
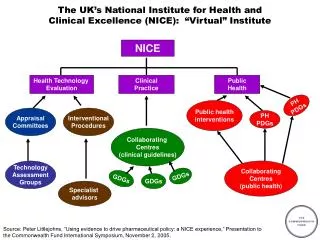
6. This flowchart sets out where our information goes to. The horizon scanning input is on the far right of the slide feeding into the Department of Health�s Advisory Committee for Topic Selection (ACTS). The group considers technologies put forward for technology appraisal (guidance) as well as proposals for clinical guidelines. This flowchart sets out where our information goes to. The horizon scanning input is on the far right of the slide feeding into the Department of Health�s Advisory Committee for Topic Selection (ACTS). The group considers technologies put forward for technology appraisal (guidance) as well as proposals for clinical guidelines.
7. ACTS membership DoH policy teams
NICE
Strategic HA
PCT
Hospital & mental health trusts
Medical, nursing & allied professions Patient groups
ABHI & ABPI
HTA experts
Welsh Assembly
Scotland
Observers: NHSC, NPC etc.
8. Recommendations from the committee are considered by the Joint Planning Group (for overall priority, NICE workload and timetabling issues) and recommendations made to Ministers. There is an interplay between JPG, NICE and Ministers before the list for consultation is published.
Other inputs include topics from the SIFT panel which considers suggestions from NHS staff and others.
The slide builds to show where industry is, or can become involved in the process.
Recommendations from the committee are considered by the Joint Planning Group (for overall priority, NICE workload and timetabling issues) and recommendations made to Ministers. There is an interplay between JPG, NICE and Ministers before the list for consultation is published.
Other inputs include topics from the SIFT panel which considers suggestions from NHS staff and others.
The slide builds to show where industry is, or can become involved in the process.
9. Company relationships Positive/Benefits
One contact point
Timely discussion of pipeline & new indications
Timing of guidance
Plan work within company Negative/Difficulties
Small US companies
Companies in �difficulties� & job moves
�Head-office�
Late communication
Lead time & delays
Miss altogether
New indications
10. Topic selection - sources Focussed routine scanning
collaborators - national & international
news sources
industry
Specialty review
Clinical experts & professional societies
Special request Our identification processes involve working with collaborators such as the UK Medicines Information regional pharmacists, scanning the internet and media, talking to industry about products in the pipeline, and working with clinicians.
We allocate each clinical area some concerted time every 2 or 4 years when we work with clinical groups such as the Royal Colleges to identify any technologies that may meet the prioritisation criteria.
Specifically in oncology we have discussions with the DoH cancer policy team, the cancer Director, the National Cancer Research Network � where we are hoping to use the clinical study groups for identification as well as prioritisation. Our identification processes involve working with collaborators such as the UK Medicines Information regional pharmacists, scanning the internet and media, talking to industry about products in the pipeline, and working with clinicians.
We allocate each clinical area some concerted time every 2 or 4 years when we work with clinical groups such as the Royal Colleges to identify any technologies that may meet the prioritisation criteria.
Specifically in oncology we have discussions with the DoH cancer policy team, the cancer Director, the National Cancer Research Network � where we are hoping to use the clinical study groups for identification as well as prioritisation.
11. Information for initial prioritisation Phase II or III trials
Quarter/year of possible licensing
Likely patient indications
Reporting date of ongoing trials
View of company of potential impact
12. Prioritisation Innovation for the patient group
And one or more significant:
patient group size & mortality & morbidity
potential for clinical benefit
potential for high cost
service reorganisation or training
inappropriate speed of adoption
13. Technology briefing Technology, marketing plans and timing
Patient indications, patient group size, epidemiology
Current treatment, service usage
Current guidance and guidelines
Research evidence
Ongoing research
Assessment of clinical and resource impact Once we are fairly certain that a technology will meet the selection criteria we begin the process of writing a technology briefing. This involves identifying and accessing information on the above.
Each technology briefing is sent to the relevant commercial developer and to 1 or 2 clinical experts who are either involved in clinical trials or are interested in the field.
The information in our briefings can become out-of-date very rapidly. So updating is sometimes requested by the DoH before a final decision is taken to recommend the topic for NICE.
Once we are fairly certain that a technology will meet the selection criteria we begin the process of writing a technology briefing. This involves identifying and accessing information on the above.
Each technology briefing is sent to the relevant commercial developer and to 1 or 2 clinical experts who are either involved in clinical trials or are interested in the field.
The information in our briefings can become out-of-date very rapidly. So updating is sometimes requested by the DoH before a final decision is taken to recommend the topic for NICE.
14. Technology briefings by specialty We have written twice as many briefings on new oncology products � mostly drugs than any other clinical area. We have written twice as many briefings on new oncology products � mostly drugs than any other clinical area.
15. NHSC input to NICE waves Each of the technology appraisal waves has had a significant input of topics from the NHSC.Each of the technology appraisal waves has had a significant input of topics from the NHSC.
16. ACTS: selection criteria for NICE Would guidance promote best possible improvement in health care:
clinical or Government priority area
significant health benefit
improve patient and carers quality of life
impact on NHS and/or societal resources
opportunity to free up resources
Is NICE able to add value? Here are the current selection criteria for ACTS in selecting topics for NICE guidance.
Here are the current selection criteria for ACTS in selecting topics for NICE guidance.
17. Challenges in horizon scanning Labour intensive
Value judgements and the �enthusiast�
Lack of information - timeliness vs accuracy
Technology & policy interaction
Some areas very difficult to predict eg oncology & new indications
�Wild cards� Labour intensive - too many development to list and assess them all. Many technologies will not reach the market.
Value judgements � we tend to deal with the �enthusiast�
Lack of information � potential benefit, cost, knock-on effects.
Policy decision - the estimation of the timing and speed of impact for all types of development but particularly non-pharmaceuticals is difficult. Technologies that require a major capital investment or increase in staff time such as some diagnostic or radiotherapy modalities, although promising, may have little or no impact until local or national policy decisions are taken.
Difficult areas � oncology, new indications: speed of licensing
�Wild cards�Labour intensive - too many development to list and assess them all. Many technologies will not reach the market.
Value judgements � we tend to deal with the �enthusiast�
Lack of information � potential benefit, cost, knock-on effects.
Policy decision - the estimation of the timing and speed of impact for all types of development but particularly non-pharmaceuticals is difficult. Technologies that require a major capital investment or increase in staff time such as some diagnostic or radiotherapy modalities, although promising, may have little or no impact until local or national policy decisions are taken.
Difficult areas � oncology, new indications: speed of licensing
�Wild cards�
18. Challenges - Oncology Number of products & wastage
Indications
Change from 3rd line usage to 1st line
Combinations & comparators
Overseas drug developers
Non-drug developments There are many challenges to horizon scanning but some are more pertinent to the oncology field. These challenges include the number of products in clinical development; the numerous indications under trial for a each new drug; movement from 2nd or 3rd line therapy to 1st line, as well as use as mono- or combination therapy.
The multiple indications and combinations ensure that there are far more developments than can be managed by the current appraisal systems and the Horizon Scanning Centre�s job is to select those most likely to make a major impact or require additional evaluation of benefit. Inevitably our decisions may prove to be inaccurate over time as more data becomes available. There are many challenges to horizon scanning but some are more pertinent to the oncology field. These challenges include the number of products in clinical development; the numerous indications under trial for a each new drug; movement from 2nd or 3rd line therapy to 1st line, as well as use as mono- or combination therapy.
The multiple indications and combinations ensure that there are far more developments than can be managed by the current appraisal systems and the Horizon Scanning Centre�s job is to select those most likely to make a major impact or require additional evaluation of benefit. Inevitably our decisions may prove to be inaccurate over time as more data becomes available.
19. NICE: Background New high cost technologies (e.g. beta interferon for MS @ �10k per patient per annum)
Uneven unfair access (postcode prescribing)
UK slow adopter of new technologies
�Faster Access to Effective Treatments�: more likely with 50% rise in UK public health spend 2000-8
Recommendations based on �clinical and cost effectiveness�
20. Four Roles for NICE Health Technology Assessment leading to Guidance
Guidelines for treatment of diseases or patient groups
Interventional procedures (classifying, registering use)
Clinical audit (Four Confidential Enquiries)
Balance: 1) and 2) central, 3) & 4) inherited
21. NICE guidance on health technologies �clinical effectiveness� uses systematic reviews of published research, hierarchy of evidence and meta analysis
Cost effectiveness in terms of �/QALY from NHS perspective
Modelling synthesises clinical and cost effectiveness, and generalise/extrapolate
No threshold for incremental �/QALY but increased attention over �20k and esp. over �30k
22. Appraisal Committees (AC): process ACs (3) �appraise� �assessments� using judgement
ACs include technical experts (clinical, health economics, statistics) and lay members
AC draft guidance is put to consultation leading to final guidance
Stakeholders (sponsor companies, patient groups, clinical bodies) can appeal (�process, perversity, or powers�)
recommendations all cite evidence of clinical benefits and often, relative cost effectiveness
23. Best Clinical Practice: role of NICE This is the cycle of appraisal and implementation described in the white paper �A First Class Service � Quality in the new NHS�. The yellow circle defines the activities originally to be undertaken within NICE. Recently NICE has become more involved in the implementation of its guidance.This is the cycle of appraisal and implementation described in the white paper �A First Class Service � Quality in the new NHS�. The yellow circle defines the activities originally to be undertaken within NICE. Recently NICE has become more involved in the implementation of its guidance.
24. NICE�s technology guidances: first five years 75 guidances, 127 technology/patient groups
NICE: few �No�s: 13/127 or 13%
Yes: 21/127 or 21%
Yes with restrictions: 89/127 or 70%
ICERs quoted for 70 tech/groups: controversial if cost/QALY > �30k
25. Review of topics with high cost per QALY Relatively few
Key decision was No to beta interferon/glaimer in MS, �40-90k per QALY.
Commissioned new data and modelling
Recommended Govt attention to pricing
Govt established �risk sharing scheme� with payment (at reduced prices) linked to success,
Model used to set patient benchmarks based on cost/QALY at �36k over 20 years.
26. Role of models when ICER>�20k �Above an ICER of �30k/QALY, the case for supporting the technology on these factors has to be increasingly strong� (NICE)
Models typically used to explore different options (who, how long, dose or combination)
27. Example: imatinib and CML High cost drug (�20k) for chronic myeloid leukemia (Phil+ chrom.) � extends life
Guidance 50 � restricted use for chronic phase. Pro use in accelerated & blast phases
Guidance 70 � extended use to chronic phase.
Due to change comparator from low cost hydoxurea to high cost interferon alpha
28. Implementation of NICE guidance Increasing concern for NICE
Research (see www.nice.org) shows take up less than expected for some technologies
But higher than expected for others
NICE has established a director of implementation
NICE guidance will be inspected by Health Commission
29. Conclusions NHSC/NICE enable NHS to identify and appraise new technologies
Using best available research on clinical and cost effectiveness
Backed up by NICE guidance to implement
Represents major shift in how NHS puts research on new technologies into practice
Lots of challenges re value judgments, measurement of health and implementation�..but a big step forward
30. NHSC contact details NHSC - www.publichealth.bham.ac.uk/horizon
NICE www.nice.org
Health Economics Facility:
http://www.hsmc.bham.ac.uk/hef/