Download
1 / 68
680 likes | 1.31k Views
Erythema and Urticaria. August 31, 2004. Flushing. Transient, diffuse redness of face/neck/trunk Niacin, Calcium Channel Blockers, cyclosporine, chemotx, vancomycin, bromocriptine, contrast dye, tamoxifen, leuprolide acetate, high dose methylprednisolone

E N D
Erythema and Urticaria August 31, 2004
Flushing • Transient, diffuse redness of face/neck/trunk • Niacin, Calcium Channel Blockers, cyclosporine, chemotx, vancomycin, bromocriptine, contrast dye, tamoxifen, leuprolide acetate, high dose methylprednisolone • Capsaicin (red pepper), sodium nitrate, sulfites, alcohol, food poisoning (ciguatera, scrombroid) • Carcinoid, Mastocytosis, Pheochromocytoma • Menopause, oophorectomy
Erythema Palmare Hypothenar erythema Elevated Estrogen Cirrhosis Metastatic Liver CA Pregnancy
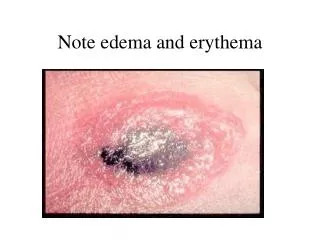
Erythema Toxicum Neonatorum Occurs in most healthy full term newborns, usually on 2nd - 3rd day. Multiple papules that rapidly evolve into pustules with an erythematous base Lesions may become confluent, especially on the face No fever, gone by 10th day DDx: Miliaria, Herpes, Bacterial folliculitis, scabies Pustule smear revealing eosinophils is diagnostic. Bx shows follliculitis with eosinophils and neutrophils
Erythema Multiforme Minor • AKA Herpes Simplex-Associated EM (HAEM) • Minor is typically associated with orolabial HSV • Major (SJS) is associated with sulfonamides, NSAIDS, antibiotics, allopurinol, Mycoplasma pneumoniae, anticonvulsants, and radiation • Cause not identified in 20% of cases • Self-limited, recurrent, young adults, spring/fall • Mild or no prodrome lasting 1-4 weeks • Lesions evolve over 24-48 hours • “Target” or “iris” lesions are diagnostic
1) Central dusky purpuric area2) Elevated edematous pale ring3) Surrounding macular erythema
EM: Vacuolar interface with “tagging” of lymphocytes along DEJ with necrotic and apoptotic keratinocytes Cytoid Bodies
Erythema Multiforme Minor • Locations: dorsal feet, limbs, elbows, knees, palms and soles • EMM appears 1-3 weeks after the herpes lesion • Tx: Self-limited, supportive care • If HSV: antivirals improve/steroid worsen; sunblock • If SJS or TEN, stop suspect medications, admit to burn unit, IVIG, steroids, etc.
Oral Erythema Multiforme • Usually limited to orolabial involvement • Concomitant skin involvement in 25% • Tongue, gingiva and buccal mucosa are the most severly affected • Erosions +/- pseudomembrane • Important to r/o Candida, because topical antifungal therapy leads to improvement in 40% of cases in which Candida is found, otherwise prednisone
Erythema Annulare Centrifugum • Most common gyrate erythema • Unknown pathogenesis • Polycyclic, trailing scale at inner border • Eccentric growth 2-3mm per day • Asymptomatic but chronic, recurrent • Evaluate for Tinea • Recommended: Good H&P, CBC, LFT’s, UA and CXR to r/o internal cancer • Responsive to topical steroids
EAC: “coat in sleeve” = lymphos tightly associated with vessels
Erythema Gyratum Repens • Rare • Undulating bands of slightly elevated wavy erythema over the entire body • “Wood grain” with “trailing scale” • Severe pruritis; eosinophilia often found • 80% underlying malignancy, MC lung CA • Rash may precede CA by 9 months • Remove CA, rash resolves
Erythema Gyratum Repens “WOOD GRAIN” APPEARANCE
Annular Erythema of Infancy • Rare • Lesions are transitory, last 36-48 hours • Onset: 6 months, resolves by 11 months without treatment
Necrolytic Migratory Erythema • AKA Glucagonoma Syndrome • Associated with amino precursor and uptake decarboxylation (APUD) tumor of the pancreas • Increased glucagon, decreased zinc • Pancreas scan may be normal • Location: periorificial, flexural, acral • Papulovesicular lesions coalesce, form pustules then erode. Active erythematous gyrate or circinate borders with central confluence • Patients present ill, with hyperglycemia, weight loss, diarrhea, anemia, atrophic glossitis, angular cheilitis • Tx: removal of tumor
Acanthosis with upper epidermal necrolysis. There is a pallor of the keratinocytes in the granular layer due to intracellular edema, thus “loss” of the granular cell layer. Edema correlates with vesicles. NME path identical to Zinc Defic.
Erythema Brucellum • Vets and Cow tenders • Starts with itching and erythema of the upper extremities, sometimes face and neck, then skin thickens and erupts with conical follicular papules • Resolves without Tx in 2 weeks • Brucella organisms not identified in lesions, suggesting a sensitization phenomenon
Recurrent Granulomatous Dermatitis with Eosinophilia • Clinical hybrid between cellulitis and urticaria • Recurrent • Reaction pattern to many possible things, including bites, onchocerciasis, parasites, varicella, mumps, tetanus immunization, drug reactions, myeloproliferative dz, atopic diathesis, hypereosinophilic synd., fungal infection • TX: OAH, TCN, UVB, PUVA, Dapsone, Prednisone low dose
Recurrent Granulomatous Dermatits with Eosinophilia • AKA Eosinophilic Cellulitis, Well’s Syndrome
Dermal eos and histiocytes surrounding central masses of brightly pink collagen that has lost its fibrillar appearance and is more amorphous “FLAME FIGURES”
Young adult women Crops of bilateral deep tender nodules, pretibial Overlying skin shiny, red Acute onset with arthralgia, malaise, edema In 2-3 days, lesions flatten and have a bruised appearance; may last days or weeks Erythema Nodosum
Erythema Nodosum in Sarcoid • MC nonspecific cutaneous finding in sarcoidosis • Young females • Anterior shins • Good prognosis • Lofgren’s Syndrome = EN with fever, arthralgias, hilar adenopathy, & fatigue
Erythema Nodosum • Reactive Process • Strep, Yersinia, Salmonella, Shigella, Coccidiomycosis, Histoplasmosis, Sporotrichosis, Blastomycosis, Toxoplasmosis, TB, Sarcoidosis, Hematologic Malignancies, Pregnancy, Oral contraceptives • HISTO: Septal panniculitis
MAY BURN, BUT DO NOT ITCH PATHERGY
Sweet's syndrome, or acute febrile neutrophilic dermatosis, is a condition characterized by the sudden onset of fever, leukocytosis, and tender, erythematous, well-demarcated papules and plaques. • 71% no known disease • 11% hematologic disease (including leukemia) • 16% immunologic disease (rheumatoid arthritis, inflammatory bowel disease) • 2% pregnancy • TX: systemic corticosteroids • The overlap between sweets and pyoderma gangrenosum well documented
Marshall’s Syndrome • Skin lesions that resemble Sweet’s but is followed by Cutis Laxa changes • Primarily, affects children • Small red papules expand to urticarial targetoid plaques with hypopigmented centers • Eosinophilic infiltrate may be seen • Biopsies demonstrate loss of elastin
Marked diminution of elastic fibers in lower dermis (Verhoeff-van Gieson stain)
Pyoderma Gangrenosum • Pathergy, as in Sweet’s Syndrome • Heal with atrophic scars • Extremely painful • 50% of pts have associated disease • MC: Crohn’s and Ulcerative Colitis • 1/3 of PG patients have arthritis • Other associations: leukemia, myeloma, polycythemia vera, Hep C, SLE, HIV, pregnancy, Takayasu’s arteritis
Pyoderma Gangrenosum ulcers with distinct rolled edges, sharply marginated, undermined blue to purple borders
Pyoderma Gangrenosum • Histopathology is not helpful • Must rule out deep fungal, mycobacterial, gummatous syphillis, synergistic gangrene, amebiasis • Biopsy with special stains and cultures are very important • cANCA to rule out Wegener’s granulomatosis
TX: Pyoderma Gangrenosum • Excise colon segment for IBS, UC, Crohn’s • Rule out/treat malignancy or infection • Steroids: topical, IL or oral depending on severity and aggressiveness • Topical 4% cromolyn or tacrolimus • Hyperbaric oxygen leads to rapid pain relief • Cyclosporine, Sulfasalazine, Dapsone, Clofazimine, Azathioprine, Mycophenolate, IVIG, Plasma exchange
History is Key • Illness: e.g., fever, sore throat, cough, rhinorrhea, vomiting, diarrhea, headache -- INFECTIOUS: STREP, HEP C, H. PYLORI • Medications: ACE inhibitors, which result in angioedema, as well as anesthetics, penicillins, cephalosporins, sulfas, diuretics, aspirin, nonsteroidal anti-inflammatory drugs [NSAIDs], iodides, bromides, quinidine, chloroquine, vancomycin, isoniazid, antiepileptic agents • Travel: rule out amebiasis, malaria, helminthics • New foods: e.g., shellfish, fish, eggs, cheese, chocolate, nuts, berries, tomatoes, alcohol • Perfumes, detergents, lotions, creams, or clothes • Exposure to new pets (dander), dust, mold, chemicals, or plants • Pregnancy (PUPPP) • Contact with nickel (eg, jewelry, jean stud buttons), rubber (eg, gloves, elastic bands), latex, industrial chemicals, and nail polish • Sun exposure or cold exposure, exercise
Urticaria Pathogenesis • Increased capillary permeability, which allows proteins and fluids to extravasate • Due to histamine release from mast cells degranulating, which in turn recruits eosinophils, neutrophils and basophils • Other triggers are leukotrienes (slow reacting substances of anaphylaxis), prostaglandins, proteases, bradykinins
Chronic Urticaria • 1/3 of these patients have circulating functional histamine-releasing autoantibodies that bind to the high-affinity IgE receptor producing mast cell-specific histamine releasing activity • Fc epsilon RI
H&E: collagen bundles separated by edema, perivascular infiltrate
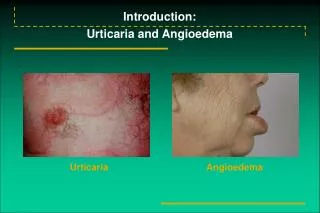
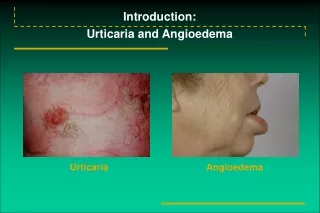
Urticaria & Angioedema DDx: • Clinical diagnosis • DDx: Urticarial Vasculitis, Bullous Pemphigoid, GA, Sarcoidosis, CTCL • Most of the diseases listed above have lesions that last longer than 24 hours • Biopsy urticarial lesions that last > 24 hours
Urticaria Evaluation • Dental and sinus x-rays can be of benefit • Order laboratory tests based only on symptoms and signs from H&P including: TSH, LFTs, Hepatitis panel, ANA, CBC • Eosinophilia: search for parasites • Food skin tests
Urticaria Treatment • Tx: OAH, multiple if necessary • Simons et al., randomized, double blind parallel series of 23 “refractory” urticarias found 58% of patients preferred H1 + H2 combinations • Atarax + Tagamet much better than Zyrtec and Tagamet • Cool bathing • Pramoxine, Sarna • Oral steroids rarely helpful
Urticaria Treatment • Foods to avoid: Fish and shellfish • Pork • Garlic, onions • Mushrooms • Tomatoes, melons, strawberries, citrus fruits, pickles and relishes • Nuts, peanuts, cheese • Remove suspected food x 3 weeks then resume
Anaphylaxis • Acute, life threatening • urticaria/angioedema 90%, SOB 60% • Onset: peak severity within 5-30 minutes • MC causes of serious anaphylactic reactions are: antibiotics, especially PCNs, NSAIDS, radiographic contrast dyes • 2nd MC cause – hymenoptera, shellfish
Anaphylaxis • Mortality rate less than 10% • Still account for vast majority of fatal reactions, peak onset 5-30 minutes • One of every 2700 hospital patients • 500 annual fatalities • Tx: 0.3 - 0.5mL dose of 1:1000 dilution of epinephrine SQ q 10-20 minutes • IV Solumedrol 50mg q6h x 2-4 doses • Benadryl, aminophyliine, neb. metaproterenol, O2, glucagon, intubation, IVFs
Hereditary Angioedema • 2nd to 4th decade, +Family history, Autosomal Dominant • May occur q 2 weeks, lasting 2 to 5 days • Eyelid and lip involvement NOT SEEN • Face, hands, arms, legs, genitals buttocks, stomach, intestines, bladder affected • N/V, colic, may mimic appendicitis • Triggers: minor trauma, surgery, sudden changes in temperature or sudden emotional stress • Presence of urticaria rules out HA
Hereditary Angioedema • AKA Quincke’s Edema • NO PRURITIS OR URTICARIA, +PAIN • Low C4, C1, C1q, C2 levels • Low or dysfunctional plasma C1 esterase inhibitor protein • 25% of deaths are from laryngeal edema • Tx of choice: fresh frozen plasma, stanazol, tranexamic acid