Download
1 / 1
10 likes | 100 Views
Comparison of preparation of infusion bags on the ward or in the pharmacy C Anton 1 , N Langford 1 , CJ Poole 2 , PA Routledge 3 , A Hutchings 3 , DN Bateman 4 , T Sheehan 5 , RE Ferner 1 1 . West Midlands Centre for Adverse Drug Reaction Reporting, City Hospital, Birmingham B18 7QH

E N D
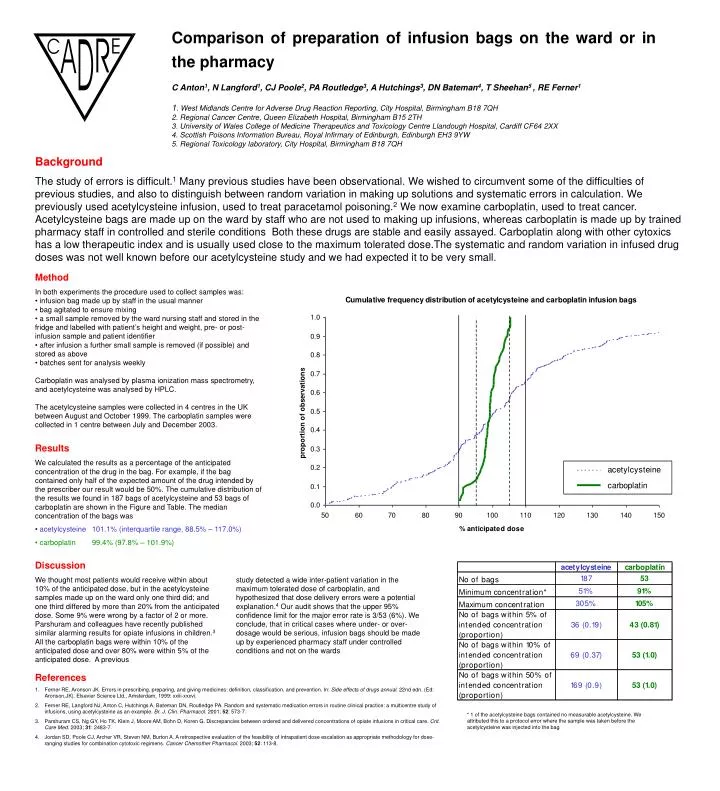
Comparison of preparation of infusion bags on the ward or in the pharmacy C Anton1, N Langford1, CJ Poole2, PA Routledge3, A Hutchings3, DN Bateman4, T Sheehan5 , RE Ferner1 1. West Midlands Centre for Adverse Drug Reaction Reporting, City Hospital, Birmingham B18 7QH 2. Regional Cancer Centre, Queen Elizabeth Hospital, Birmingham B15 2TH 3. University of Wales College of Medicine Therapeutics and Toxicology Centre Llandough Hospital, Cardiff CF64 2XX 4. Scottish Poisons Information Bureau, Royal Infirmary of Edinburgh, Edinburgh EH3 9YW 5. Regional Toxicology laboratory, City Hospital, Birmingham B18 7QH Background The study of errors is difficult.1 Many previous studies have been observational. We wished to circumvent some of the difficulties of previous studies, and also to distinguish between random variation in making up solutions and systematic errors in calculation. We previously used acetylcysteine infusion, used to treat paracetamol poisoning.2 We now examine carboplatin, used to treat cancer. Acetylcysteine bags are made up on the ward by staff who are not used to making up infusions, whereas carboplatin is made up by trained pharmacy staff in controlled and sterile conditions Both these drugs are stable and easily assayed. Carboplatin along with other cytoxics has a low therapeutic index and is usually used close to the maximum tolerated dose.The systematic and random variation in infused drug doses was not well known before our acetylcysteine study and we had expected it to be very small. • Method • In both experiments the procedure used to collect samples was: • infusion bag made up by staff in the usual manner • bag agitated to ensure mixing • a small sample removed by the ward nursing staff and stored in the fridge and labelled with patient’s height and weight, pre- or post-infusion sample and patient identifier • after infusion a further small sample is removed (if possible) and stored as above • batches sent for analysis weekly • Carboplatin was analysed by plasma ionization mass spectrometry, and acetylcysteine was analysed by HPLC. • The acetylcysteine samples were collected in 4 centres in the UK between August and October 1999. The carboplatin samples were collected in 1 centre between July and December 2003. • Results • We calculated the results as a percentage of the anticipated concentration of the drug in the bag. For example, if the bag contained only half of the expected amount of the drug intended by the prescriber our result would be 50%. The cumulative distribution of the results we found in 187 bags of acetylcysteine and 53 bags of carboplatin are shown in the Figure and Table. The median concentration of the bags was • acetylcysteine 101.1% (interquartile range, 88.5% – 117.0%) • carboplatin 99.4% (97.8% – 101.9%) Discussion We thought most patients would receive within about 10% of the anticipated dose, but in the acetylcysteine samples made up on the ward only one third did; and one third differed by more than 20% from the anticipated dose. Some 9% were wrong by a factor of 2 or more. Parshuram and colleagues have recently published similar alarming results for opiate infusions in children.3 All the carboplatin bags were within 10% of the anticipated dose and over 80% were within 5% of the anticipated dose. A previous study detected a wide inter-patient variation in the maximum tolerated dose of carboplatin, and hypothesized that dose delivery errors were a potential explanation.4 Our audit shows that the upper 95% confidence limit for the major error rate is 3/53 (6%). We conclude, that in critical cases where under- or over-dosage would be serious, infusion bags should be made up by experienced pharmacy staff under controlled conditions and not on the wards • References • Ferner RE, Aronson JK. Errors in prescribing, preparing, and giving medicines: definition, classification, and prevention. In: Side effects of drugs annual. 22nd edn. (Ed: Aronson,JK). Elsevier Science Ltd., Amsterdam, 1999: xxiii‑xxxvi. • Ferner RE, Langford NJ, Anton C, Hutchings A, Bateman DN, Routledge PA. Random and systematic medication errors in routine clinical practice: a multicentre study of infusions, using acetylcysteine as an example. Br. J. Clin. Pharmacol. 2001; 52: 573-7. • Parshuram CS, Ng GY, Ho TK, Klein J, Moore AM, Bohn D, Koren G. Discrepancies between ordered and delivered concentrations of opiate infusions in critical care. Crit. Care Med. 2003; 31: 2483-7. • Jordan SD, Poole CJ, Archer VR, Steven NM, Burton A. A retrospective evaluation of the feasibility of intrapatient dose escalation as appropriate methodology for dose-ranging studies for combination cytotoxic regimens. Cancer Chemother Pharmacol. 2003; 52: 113-8. * 1 of the acetylcysteine bags contained no measurable acetylcysteine. We attributed this to a protocol error where the sample was taken before the acetylcysteine was injected into the bag