Download
1 / 36
700 likes | 6.86k Views
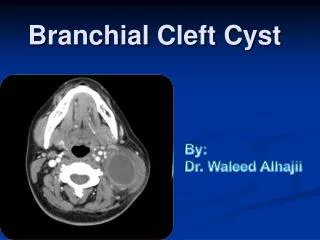
Branchial Cleft Cyst. By : Dr. Waleed Alhajii. What is a Branchial Cyst?. Definition: Congenital epithelial cysts , which arise on the lateral part of the neck due to failure of obliteration of the second branchial cleft in embryonic development. .

E N D
Branchial Cleft Cyst By: Dr. WaleedAlhajii
What is a Branchial Cyst? Definition: Congenital epithelial cysts, which arise on the lateral part of the neck due to failure of obliteration of the second branchial cleft in embryonic development.
Branchila cleft cyst = Lymphoepithelial cyst “Lymphatic origin, Modern Theory” • The name branchial means in Greek “Gill” , Those structures are responsible of development of Gills in fish. “Classic Theory” • Commonest cysts to arise in the neck.
Classical location • Anterior to the sternocleidomastoid muscle. • However there have been a number of case reports describing cysts which were found in areas other than the classical position.
Etiology • Many theories • They can be grouped into two categories: • the congenital • The cervical lymph nodes cystic transformation theories.
Easier approach to Embryology • Structures between the developing head and the heart (i.e., the face, neck, oropharynx, and the larynx) develop from the branchial apparatus. • There are six branchial arches; the last two are rudimentary. • Each arch has a bar of mesoderm.
Caudal to each of the four arches is an internal pouch lined with entoderm. • Externally is branchial cleft, lined with ectoderm. • Between each bar, a branchial plate, composed of entoderm and ectoderm, separates the branchial cleft from the branchial pouch.
Anatomical Considerations • The second arch grows downwards and ultimately covers the third and fourth arches. • The buried clefts normally disappear around the seventh week of development. • If a portion of the cleft remains entrapped and fails to disappear, its remnants form a cyst.
Second cleft Cyst with tract extending up to Pharynx • Note tract goes between internal & external carotid arteries and close to cranial nerves IX, X, XII which control among other functions tongue movement and swallowing.
History • Solitary, painless mass in the neck of a child or a young adult. • History of intermittent swelling and tenderness of the lesion during upper respiratory tract infection may exist. • Discharge if associated with a sinus tract. • May present with locally compressive symptoms. • + family history.
Physical Examination • Primary lesion: Branchial cysts are smooth, nontender, fluctuant masses, which occur along the lower one third of the anteromedial border of the sternocleidomastoid muscle between the muscle and the overlying skin. • Secondary lesion: The lesion may be tender if secondarily inflamed or infected. When associated with a sinus tract, mucoid or purulent discharge onto the skin or into the pharynx may be present.
Diagnosis • Cyst arising off midline of the neck and having lymphoepithelial characteristics should be regarded as a branchial cyst. • Usually occur in the 2nd or 3rd decade of life. • Most commonly found in the anterior triangle of the neck anterior to the upper third of the sternomastoid. • A cyst occupying the posterior triangle is extremely rare. • Hence they should be suspected in all the cystic swellings of the neck except the median ones.
Imaging • On general principle it’s less helpful than expected • Although you can always tell where is the lesion, but differentiating between other causes of cystic neck masses is not always easy.
Ultrasound • Well defined, echogenic mass usually anterior to the carotid artery, draped anterior to the sternocleidomastoid muscle
CT • Well defined, low density unilocular mass with a thin uniformly enhancing rim
Axial contrast-enhanced CT scan shows a left-sided cyst with a thick, enhancing rim. This cyst is behind the submandibular gland, lateral to the carotid sheath structures, and deep to the anterior margin of the sternocleidomastoid muscle. There is an enhancing tract (arrow) extending from the cyst toward the left palatine tonsil. This was an infected second branchial cleft cyst with an internal tract. Such a tract typically passes between the internal and external carotid arteries and ends in the palatine tonsil.
MRI • MRI allows for finer resolution during preoperative planning. The wall may be enhancing on gadolinium scans.
Differential Diagnosis • Branchiogenic carcinoma • Tuberculous adenitis • Lipoma • Metastatic malignant neoplasms (SCCA from a primary site in the aerodigestive tract) • Cystic hygroma (lymphangioma) • Carotid body tumors • Lymphomas • Hemangiomas • Thyroid cysts • Ectopic thyroid • Cervical thymic cysts • Thyroglossal duct cyst • Parotid cystic tumors
Axial contrast-enhanced CT scan shows a well-delineated fatty mass in the subcutaneous tissues of the back of the neck. Branchial cleft cyst
Cystichygroma Cysticlymphangioma Branchial cleft cyst
Parotid, malignant tumors. Axial T1-weighted MRI with fat saturation and contrast enhancement shows an enhancing mass extending into the superficial and deep lobes of the right parotid gland. Pathology indicated a squamous cell carcinoma. Branchial cleft cyst
T1-Weighted MRI. A well defined mass is present along theanterior triangle of the neck on the right side. There are low signal regionswithin this mass suggesting the presence of calcifications and flow-voids (arrows). T2-Weighted Axial Images Through the Submandi-bular Region. The mass is bright on T2-weighted images and again exhibits focal lucencies compatible with flow voids. Contrast Enhanced MR in the Axial Plane.There is bright enhancement of the mass. Flow voidsproduce a "salt and pepper" appearance. Paragangliomas
Axial contrast-enhanced CT scan shows a well-delineated irregular mass lesion taking early KM enhancment Branchial cleft cyst Hemangioma
Treatment • The treatment of branchial cleft cysts is surgical excision.
This branchial cleft cyst was followed superiorly to the region of the oropharynx, but no communication was found. The picture below shows the anatomy of the carotid triangle after removal of the cyst.
Thank You Marina Waves, Salmiya Waterfront, Kuwait