Download
1 / 22
230 likes | 377 Views
Systematic Review Presentation. Jill Collins, RN, BSN Jerilyn Rodgers, RN, BSN NU 517 Clinical Scholarship for EBP September 23, 2010. PROBLEM AND PURPOSE. Clinical Question addressed:

E N D
Systematic Review Presentation Jill Collins, RN, BSN Jerilyn Rodgers, RN, BSN NU 517 Clinical Scholarship for EBP September 23, 2010
PROBLEM AND PURPOSE • Clinical Question addressed: How does interprofessional collaboration (IPC) effect the delivery of health services in patient care? IPC, as defined by the authors of this review, is “the process in which different professional groups work together to positively impact healthcare” (pg. 2) • Purpose of this systematic review: “To assess the impact of practice-based interventions designed to change IPC, compared to no intervention or to an alternative intervention, on one or more of the following primary outcomes: patient satisfactions and/or the effectiveness and efficiency of the health care provided” (pg 1).
SAMPLE SELECTION PROCESS • Search processes used: > Cochrane Effective Practice and Organization of Care Group Specialized Register (2000-2007) >MEDLINE (1950-2007) >CINAHL (1982-2007) >Hand search of the Journal of Interprofessional Care (1999 to 2007) >Reference list of included studies
Sample Selection (cont) • The data bases utilized in the review were appropriate and comprehensive. The authors used multiple computer databases as well as hand searched a related journal and utilized the reference list of the included studies. • According to Melnyk and Fineout-Overholt the utilization of these resources ensures that “research findings from all relevant disciplines and in all languages are found” (2010, pg. 123).
Sample Selection (cont) • Inclusion criteria: 1. ”A practice-based IPC intervention occurred” (pg 5). 2. “Interprofessional practice, care process, patient health or patient or family satisfaction outcomes were reported” (pg 5). 3. “The intervention was evaluated using RCT design” (pg. 5).
Sample Selection (cont.) • 1128 abstracts were retrieved in the searches and were reviewed independently by at least two of the three authors. • After initial evaluation, 77 studies potentially met the inclusion criteria. This was narrowed to five after complete and thorough review by all three authors. • Exclusion criteria: Studies which did not include practice-based IPC interventions or did not have an appropriate outcome.
QUALITY APPRAISAL • The researchers used the defensible and well defined set of criteria as recommended by the Cochrane Effective Practice and Organization of Care Group (EPOC) to assess risk of bias of all studies. • These criteria included (pg 5) : • Concealment of allocation • Follow-up of professionals • Follow-up of patients or episodes of care • Blinded assessment of primary outcome(s) • Baseline measurement • Reliable primary outcome measure(s) • Protection against t contamination
Quality Appraisal (cont.) • An overall quality rating was assigned to each study to evaluate the methodological quality of protection against bias. These ratings were clearly outlined and included: > High: “all criteria rated as done (or not applicable)” (pg. 5). > Moderate: “one or two criteria were not done or unclear” (pg. 5). > Low: “three or more criteria were not done or unclear” (pg. 5). Of the five studies, one was ranked as high quality and the other four were ranked as moderate quality
DATA ANALYSIS • The following data was extracted from each study (pg. 5): • Study setting (country, healthcare setting) • Types of study participants • Description of collaborative intervention • Description of any other intervention • Main outcome measures • Results for the main outcome measures • Any additional information that potentially effected the results
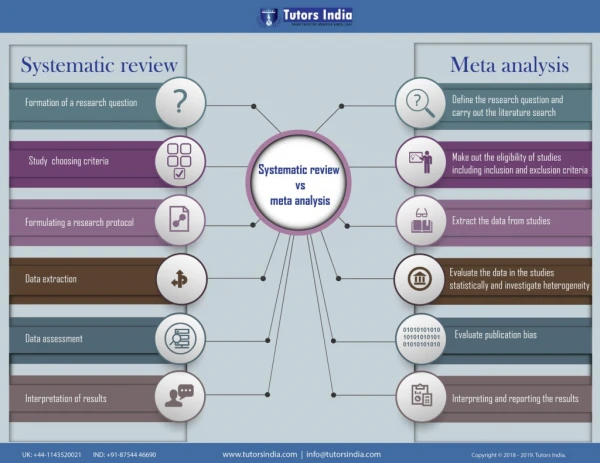
Data Analysis (cont.) • Aggregate data was used in this analysis. The review analyzed the effect of ICP processes on patient outcomes as a whole and did not review individual patient data. • The authors of this review stated “ideally we would have conducted a meta-analyses of study outcomes for this review. This, however, was not possible due to the small number of included studies and the differences in relation to methodological design and outcome measures across the study. Consequently, we have presented the results in a narrative format”(pg. 5)
RESULTS AND CONCLUSIONS Five studies were reviewed: 1)Cheater 2005 was a RCT done to evaluate “an externally facilitated program aimed at improving multidisciplinary audit” (pg. 6). Represented in the multidisciplinary team were nurses, physicians, allied professionals, service support staff, managers and a range of specialties. Primary outcome: “participation in the intervention program was associated with increased audit activity, with 9 of the 11 teams reporting improvements to care and seven teams completing the full audit cycle” (pg. 7). Level of Significance: P = 0.003, confidence interval of 99.97% for audit knowledge and P = 0.003, confidence interval 99.97% for skills. Summary: “Multidisciplinary meetings with an external facilitator, who used strategies to encourage collaborative working, was associated with increased audit activity and reported improvements to care (Cheater 2005)” (pg. 7).
Results and Conclusions (cont) 2) Curley 1998 was a RCT “examined the effects of daily interdisciplinary rounds in inpatient medical wards at an acute care hospital” (pg. 6). Represented in the teams were interns and residents in medicine, nurses, supervisor of nurses, respirologists, pharmacists, nutritionists and social workers. Primary outcome: “mean length of stay for the patients in the interdisciplinary rounds group was 5.46 days, compared with 6.06 days for traditional care” (pg. 16). “mean total charges were $6,681 and $8,090” (pg. 16) respectively for the two groups. “Regarding respiratory therapy, 91.7% of the orders for administration of aerosols in the interdisciplinary rounds group were appropriate, compared with 73.6% for the traditional rounds group” (pg. 7). Level of Significance: P = 0.006 with a confidence interval of 99.94% for length of stay. P = 0.002 with a confidence level of 99.98% for total charges. P = 0.075 with a confidence interval of 75% for administration of aerosols. Summary: “Daily interdisciplinary rounds in inpatient medical wards at na acute care hospital had a positive impact on length of stay and total charges (Curley 1998)” (pg. 7)
Results and Conclusions (cont) 3) Schmidt 1998 was a RCT to “examine monthly facilitated multidisciplinary rounds on the quality and quantity of psychotropic drug prescribing” (pg. 18). Represented in the meetings included physician, pharmacist, nurses and nursing assistants. Primary outcome: “The average numbers of drugs prescribed in the experimental homes was the same before and after the interventions” (pg. 18). “The use on nonrecommended hypnotics declined by 37% in the experimental homes versus a decrease of 3% in the control homes. There was no change in the prescribing of nonrecommended anxiolytics in the experimental homes and an increase of 7% in the control homes. Nonrecommended antidepressant drugs decreased by 59% in the experimental homes and by 34% in control homes” (pg. 18). Level of significance: P = 0.02, with a confidence interval of 98% for prescribing psychotropic drugs. P < .001, with a confidence interval of 99.9% for decreasing nonrecommended hypnotics. P < .001 with a confidence interal of 99.9% for decreasing nonrecommended antidepressant drugs for the experimental homes and P = .002, with a confidence interval of 98% in the control homes. Summary: “Monthly multidisciplinary team meetings improved prescribing of psychotropic drugs in nursing homes (Schmidt 1998)” (pg. 7).
Results and Conclusions (cont) 4) Wild 2004 was a RCT “where patients in inpatient telemetry ward in a community hospital were randomised to the intervention medical team which conducted interdisciplinary rounds or to the control team which provided standard care” (pg. 20). Represented in the meetings were physicians, nurses, case managers, pharmacists, dietitians and physical therapists. Primary outcome: “No difference in length of hospital stay between the experimental group and the control group” (pg. 20). Level of Significance: P = 0.90, with a confidence interval of 90%. Summary: “no impact on length of stay in a community hospital telemetry ward (Wild 2004)” (pg. 7).
Results and Conclusions (cont) 5) Wilson 2004 was a RCT “comparing multidisciplinary audioconferencing and multidisciplinary videoconferencing with a team that worked at two hospitals” (pg. 21). Represented in the team were medical staff specialists, medical registars, medical students, nurses, occupational therapists, social workers and speech pathologists. Primary outcome: “The mean number of audioconferences held per patient (3.3+ 4.4) was greater than the mean number of videoconferences held (1.9 + 1.3)” (pg. 21). “There was also a reduction in the average length of treatment for the videoconference group (6.0 + 4.5 days) compared to the audioconference group (10 + 12.3 days)” (pg. 21). No differences were found in the number of occasions of service between the groups, or the length of the conference between the two groups. Level of significance: P = 0.04, with a confidence interval of 96% for decreased number of case conferences. P = 0.03, with a confidence interval of 97% for a reduction in the average length of treatment. Summary: “Videoconferencing compared to audioconferencing multidisciplinary case conferences showed mixed results; there was a decrease number of case conferences per patient and shorter length of treatment but no differences in occasions of service or the length of the conference (Wilson 2004)” (pg. 7)
CONCLUSIONS DRAWN BY AUTHORS The authors feel they succeeded in locating five studies, but this remains a small number of studies. Even though the small number of studies “offer preliminary findings concerning the effectiveness of these interventions in improving healthcare processes and outcomes” (pg. 8) and some methodological limitations “preclude definitive conclusions” (pg. 8).
IMPLICATIONS • Implications for Nursing • There are multiple disciplines involved in the care of a patient from the time they present to the hospital for admission to the time they leave and even past discharge. The care the patient receives and the outcomes they have largely depend on the collaboration of these disciplines. When there is effective collaboration, patients tend to have better outcomes and satisfaction. For most patients, the nursing staff has the greatest amount of contact with them and are often responsible for their coordination of care. Therefore, the nursing staff needs to be as effective as possible in establishing IPC for their patients to provide the best possible outcomes.
Implications (cont.) • Proposed changes in practice • “the findings from the small number of studies included in this review show that practice-based interventions aimed at improving collaboration through practice changes may improve healthcare and patient outcomes. However, this is based on such a small number of studies that at this point, interventions to promote IPC should be labeled “promising” rather that “proven”” (pg. 8)
Implications (cont.) • Implications for research • Even the small amount of evidence presented in the five studies reviewed demonstrated an improvement in patient outcomes and satisfaction. There was evidence showing IPC problems that are encountered on a daily basis for health professionals. It is suggested in this review that future randomized studies have a clear focus on IPC, longer acclimatization periods prior to evaluation of newly implemented teamwork interventions and longer follow up (pg. 9). • Future research also needs to focus on the conceptualizations and measurements of collaboration. Qualitative and quantitative methods need to be utilized in each study to improve understanding of how the intervention addresses collaboration, the nature of changes in relation to it, and how this in turn leads to the outcomes achieved (pg. 9).
Implications (cont.) • Utilization of findings in nursing practice • Faced with the tough economic times that are upon us and the encouragement from administrations to do “more with less”, it will become vitally important that nurses are able to work well and communicate well with other disciplines to provide the best competent, evidence-based practice to their patients. For those nurses in positions to do so, changes need to be made in processes at their places of employment to utilize IPC more effectively. For those nurses just starting out, campaigning for change in these process as well as utilizing and communicating with other disciplines to the best of their ability will hopefully drive the change needed.
References Melnyk, B., Fineout-Overholt, E. (2011). Evidence-Based Practice in Nursing and Healthcare. Philadelphia: Wolters Kluwer Health / Lippincott Williams & Wilkins. Zwarenstein, M., Goldman, J., Reevs, S. (2009). Interprofessional collaboration: effects of practice-based interventions on professional practice and healthcare outcomes. Cochrane Database of Systematic Reviews, 3.