Download
1 / 23
470 likes | 1.25k Views
Topically Applied Corticosteroids. Dr Muhammad Raza. Topical Preparations : Products which are designed for application to the skin - either by simply spreading them over the skin or by rubbing them in.

E N D
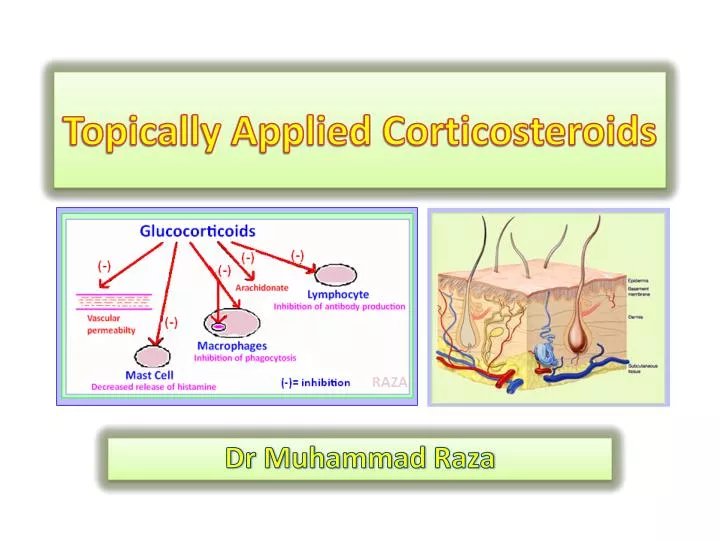
Topically Applied Corticosteroids Dr Muhammad Raza
Topical Preparations: Products which are designed for application to the skin - either by simply spreading them over the skin or byrubbing them in. • Dermatological preparations:are employed for the treatment of diseased or injured skin. Diseased, injured or inflamed skin proves more permeable than intact skin. • Percutaneous topical preparations:are intended for use on intact skin and they produce their effects either locally or systemically.
Topically used corticosteroids • The most potent and effective anti-inflammatory medications available • They are the therapy of choice in most inflammatorydiseases,pruritic eruptions (dermatitis),hyperproliferativedisorders (psoriasis),infiltrativedisorders (sarcoidosis) • Effectiveness of the drugs is due to their anti-inflammatory activity. (Explain the mechanism of action?) • They have the ability to inhibit cell division • In dermatologic diseases characterized by increased cell turnover e.g. psoriasis, the anti mitotic effect of steroids is important factor.
Anti-inflammatory action of corticosteroids PHARMACOLOGY FOR HEALTHCARE PROFESSIONALS
Analogues of topical steroids and their efficacy • Hydrocortisone (HC) is the prototype. (Active or not?) • Prednisolone & Methylprednisoloneare active as HC • 9-α-flourinatedcompounds like dexamethasone & Betamethasone (As hydrocortisone) • Attaching 5-carbon valerateto the 17 hydroxy position to betamethasone300 timesactive as hydrocortisone • Acetonide derivatives of fluorinated steroids potent topical drugs • 21-derivatives of acetonide 5-fold increase
Intrinsic activity of topical corticosteroids is dependent on chemical modification of the molecule like F at C9, carbon valerate chain at C17 • Betamethasone + 5- carbon valerate chain at 17 position > 300 times as active as hydrocortisone
Advantages of topical corticosteroids • Wide spectrum against skin diseases • Rapid action in small amounts • Ease of use (topical application) • Absence of pain or odor • Relative lack of sensitization • Prolonged stability • Compatibility with almost all commonly used topical medications • Rare systemic untoward systemic side effects
Factors affecting the effectiveness of topical corticosteroids 1.Drug potency • Active form (e.g. prednisone & prednisolone), Binding to a glucocorticoid receptor • Addition of halogen atom (e.g. fluoride) • Vehicle(Oint., cream, lotion, etc) • Added drug(salicylic acid, urea) 2.Percutaneous penetration: See next slide
PercutaneousDrug Absorption All topical preparations must make their way into the skin before they can exert effects. • Percutaneous absorption involves: • Dissolution of the drug in its vehicle, • Diffusion of the drug from the vehicle to the surface of the skin, and • The actual penetration of the drug through the different layers of the skin. • Percutaneous absorption may be effected by the following routes: • Transcellular diffusion • Diffusion through channels between the epidermal cells • Diffusion through sebaceous ducts • Diffusion through the hair follicles • Diffusion through the sweat ducts
Factors affecting trans-dermal absorption of corticosteroids • Site of steroid application. (See the next diagram) • Hydration • Long term occlusion of impermeable film. (▲100 times) • Inflamed skin. (Health status of skin) • Dosage form: ointment > cream and lotion. • Increasing the concentrationof applied cortisone. • Lipophilicity of the corticosteroids • Solubility of cortisone in the vehicle. • Intra lesionalinjection. • In diseases that are very responsive apply low to minimum efficacy corticosteroids. • In less responsive diseases apply high efficacy preparations + occlusion or both, when remission occurs shift to low efficacy corticosteroids.
Absorption of steroids is dependent on the site of their application (the times = the concentration of absorbed steroid relative to the percentage of concentration of the absorbed hydrocortisone). Skin is thinnest on the eyelids at 0.05 mm and the thickest on the palms and soles at 1.5 mm. Back 3 mm Eyelids Thin (Palm- Thick) (Scrotum-thin) (Sole- Thick)
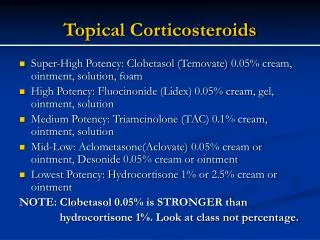
Classification of topical steroids according to their potency Hydrocortisone 1% <Betamethasonevalerate 0.1% <Clobetasole propionate 0.05% • Lowest efficacy corticosteroids:Mild • Who:infant, child, adult • Areas: Face, folds , genitals, extensive areas of the skin • Examples • Hydrocortisone (0.25 - 2.5 %). • Dexamethasone (0.1%, 0.04%). B. Low efficacy corticosteroids:(Mild to moderate) • Who:infant, child, adult • Potency: 2-25 times as hydrocortisone • Sites: Face, folds, genitals, • Examples: • Betamethasonevalerate(0.01%) • Triamcinoloneacetonide(0.025%)
Classification of topical steroids according to their potency C. Intermediate efficacy corticosteroids:Moderately potent • Potency:Up to 100 times as hydrocortisone • Who:Adult & Child & Extensive area of the skin • Examples: • Hydrocortisone valerate (0.2%) (Betnovate) • Betamethasonevalerate (0.1 %). • Triamcinoloneacetonide (0.1 %). (Kenacort) D. High efficacy corticosteroids:Potent • Who: Adults • Potency:Up to 150 times as hydrocortisone • Areas: Localized thick lesions • Examples: • Betamethasonedipropionate (0.05%) (diprolone) • Triamcinoloneacetonide (0.5%). • Flucinoloneacetonide (0.2%).
Classification of topical steroids according to their potency E. Highest efficacy corticosteroids:(Very Potent) • Who: Adult • Potency:Up to 600 times hydrocortisone • Areas:Resistant & Localized thick lesions (palm) • Examples: • Clobetasolepropionate 0.05% (Dermovate) • Betamethasonedipropionate(Diprosone) • General Notes: • Begin with high efficacy compound then maintain on that with less efficacy • Use the less potent corticosteroids e.g. 1% hydrocortisone on scrotum, groin, axillae, eyelids, face. Why?
Which preparation? cream or ointment, lotion or gel • As with moisturizers, the type of steroid formulation most suitable depends on the characteristics of disease and the area of skin affected. • Lotions and gels are most suitable for hairy areas of skin. • Creams are better for moist, weeping areas of skin, while • Ointments are most suitable for drier, scaly areas
Dermatological disorders responsive to topical corticosteroids • A. Highly responsive disorders: • 1- Atopic dermatitis. • 2- Seborrheic dermatitis. • 3- Lichen simplex chronicus. • 4- Pruritusani. • 5- Later phase of allergic contact & irritant dermatitis. • 6- Stasis dermatitis. • 7- Psoriasis (genitalia and face).
Dermatological disorders responsive to topical corticosteroids B. Less responsive disorders: • Discoid lupus erythematosus • Psoriasis of palms and soles • Necrobiosislipoidicadiabeticorum • Sarcoidosis • Lichen striatus • Vitiligo • Granulomaannulare C. Least responsive disorders: (Intra lesion injection required): • Kelosis • Hypertrophic scars • Hypertrophic lichen planus • Alopecia areata • Acne cysts • Prurigonodularis
Corticosteroids • Action • Corticoid depresses formation, release and activity of endogenous mediators of inflammation, including • PGs, • kinins, • histamine, • liposomal enzymes and • complement system. Also • modifies body's immune response • Leads to: • Inhibit. lymphoid proliferation • Lyses of either suppressor or helper T cells • Monocyte- macrophage system inhibit chemotaxis • Inhibit. of IL6 & IL1, IL2, TNF, PAF, leukotriens, PGS. • Inhibits the antibody response • Decrease amount of antibody
Topical steroids: Adverse effects I. Systemic:Extremely rare e.g. if TS >50 gmclobetasolpropionate or 500 gm of hydrocortisone/week • Potential suppression of pituitary-adrenal axis Occlusion,surface area, amount, duration, concentration, Type (Clobetasol), Infants, children, liver failure • Growth retardation in children. • Iatrogenic Cushing's syndrome. • When: Too long, too much, too often, too old, too young, too extensive, face, folds, genitalia. • What are the adverse effects of steroid ê occlusion? Infection, folliculitis, miliaria,▼ heat change, ▲sunburn, atrophy, striae Occlusive dressings (airtight dressings) absorption of the steroid and may also the chances of side effects
Topical steroids: Adverse effects II. Local:Rare if TS used correctly • Skin atrophy,striae(stretch marks), telangiectases, • Easy bruising and tearing of skin (purpura, ecchymosis). • Pustules & Papules. • Peri-oral dermatitis (rash around mouth) • Steroid acne. • ▲Susceptibility to skin infection, Mask superficial infections, worsen fungal infections. • Tachyphylaxis • Hypo-pigmentation. • Hyper-trichosis. (Excessive abnormal hair growth) • Glaucoma & cataract. (when used around the eye) • Allergic contact dermatitis.(leg ulcers, stasis )
Contraindications to topical corticosteroids • Untreated skin infections (bacterial, fungal, or viral) • Acne rosacea • Peri-oral dermatitis • Potent corticosteroids are contra-indicated in widespread plaque psoriasis. Why? Questions for revision: • What are the precautions of using topical corticosteroids in children and infants? • On which basis you choose the dosage form of corticosteroids? e.g. occlusion • How frequent you apply the topical corticosteroids per day.Why? • What is your opinion about using topical steroids in pregnancy and lactation?
How can you minimize the side effects of topical steroids? • Potency:use the leastpotent steroid whenever possible • Frequency:≱Once or Twicedaily • Amount:use steroid sparingly by using FTU. How? (1, 2, 3, 6, 7 FTU) • Duration,not for prolonged periods – change to less potent with recovery • Surface area: Broad area—least potent, and least amount, reduce frequency • Areas of skin: take care of areas that absorb more (like face and genitalia) • Occlusion: Precautions with occlusion • Once the lesion responded, reduce or stop the steroid & maintain on a mild one • Never use the steroid as moisturizers • Getting the dose right - the fingertip unit • One fingertip unit (FTU) is the amount of topical steroid that is squeezed out from a standard tube along an adult's fingertip. (This assumes the tube has a standard 5 mm nozzle) A finger tip is from the very end of the finger to the first crease in the finger.
Intralesional corticosteroids Definition: Injection of small amounts of corticosteroids into coetaneous lesions (Relatively insoluble steroids) Examples: Triamcinoloneacetonide, triamcinolonediacetate, betamethasoneacetatephosphate) 2.5 mg/ml Advantages: • High concentration • Prolonged depot (3-4 weeks) • No systemic side effects Treated diseases: Acne cysts, Alopecia areata, keloids, nail disorders, Prurigonodularis Methods:Insulin syringe (1ml/30 G), Air powered gun ( pyogenicInfection & Viral hepatitis). Dose 1mg/injection site of triamcinolone(Conc. 10mg/ml- Dose Vol. 0.1ml) Adverse efects: • No systemic.Why? • Local:Atrophy, hypo-pigmentation, hair growth, infection, ulceration.