Download
1 / 30
300 likes | 575 Views
Breast Cancer Risk and Risk Assessment Models. Jessica Ray, MS, CGC Cancer Genetic Counselor Ambry Genetic Laboratories jray@ambrygen.com. ¡Vida! Educational Series - Promoting Good Health. Learning Objectives .

E N D
Breast Cancer Risk and Risk Assessment Models Jessica Ray, MS, CGC Cancer Genetic Counselor Ambry Genetic Laboratories jray@ambrygen.com ¡Vida!Educational Series - Promoting Good Health
Learning Objectives • Identify Personal and Family Characteristics that may indicate an inherited increased risk for cancer • Understand the role of genetic counseling in assessing patients with possible hereditary cancer syndromes • Understand characteristics, advantages, limitations, and differences of the Gail and BRCAPRO risk-assessment tools used by clinicians to help establish cancer risk
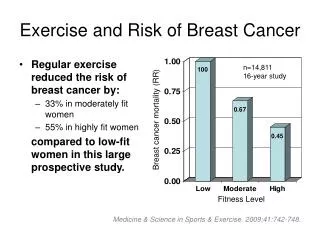
Who Is at “High Risk”? • Atypia • 5-year Gail risk >1.7% • 2 or more 2nd-degree premenopausal affected relatives • Combined estrogen-progesterone hormone therapy for more than 10 years • Mammographically dense breasts • Obesity
Who Is at “Very High Risk”? • Personal history of BC <50 • BRCA1 or BRCA2 mutation carrier • 2 or more 1st-degree relatives with BC • Lobular carcinoma in situ (LCIS) • Atypia and a 1st-degree relative with BC
What is Genetic Counseling? Genetic Counseling is a communication process that deals with both the medical and psychological issues associated with the occurrence of a genetic disorder in a family • Cancer genetic counseling focuses on hereditary cancer syndromes • This process involves one or more trained professionals to help the individual or family
Reasons for Seeking Genetics Consultation • To learn about • Personal risk for cancer • Children’s risk for cancer • Family’s risk for cancer • Risks for developing cancer if you have a “cancer gene” • Recommendations for screening, surveillance, and/or treatment • Educational information • To obtain genetic DNA testing J Med Genet 2000; 37:866-874
Key Flags that Warrant Genetic Counseling • Significant family medical history-breast, ovarian, prostate, colon, uterine, melanoma, pancreatic, or other cancers • Cancer occurs in every generation • Early age of onset (< 50 years) • Male breast cancer • Bilateral cancer, or multiple primary cancers in one individual • Known family genetic mutation • Ethnicity – Ashkenazi Jewish ancestry
Sporadic, Familial or Hereditary? • 5-10% cancers have a hereditary component • Over 200 hereditary cancer syndromes described • Hereditary cancer tends to occur at younger ages than sporadic cancer, oftenbilateral, multifocal • Lifetime risks of cancer exceed cancer risks due to noninherited factors (early menarche, nulliparity, late age of menopause, HRT, etc) • Majority show an autosomal dominant inheritance pattern (few are recessive)
Breast 41 Ovarian 40-50 Prostate 63 Breast 62 Ovarian 60 Prostate 71 Average Age of DiagnosisHereditarySporadic
Gail Model National Cancer Institute http://www.cancer.gov/bcrisktool/Default.aspx
Gail Model: Advantages • Identifies women who could benefit from preventive interventions; may assist in making clinical decisions (Determination of eligibility for tamoxifen for breast cancer risk reduction…Gail score>1.7) • Incorporates risk factors other than family history (eg, reproductive variables, atypical hyperplasia, history of breast biopsies) • Calculation of breast cancer risk in absence of family history in women • Shows that BC risk increases with age and, therefore, may prompt discussion about the importance of BC screening • Used to counsel and educate women, especially those who overestimate their BC risk
Gail Model: Limitations • Not validated for black, Hispanic, and other ethnic groups • Only solicits family history involving first-degree relatives • May underestimate risk when family history is on father’s side • Does not take into account age at which relatives developed BC • Effect of number of breast biopsies (without atypical hyperplasia) may cause inflated risk estimates • May underestimate risk for women with demonstrated mutations of the BRCA1 or BRCA2 genes
BRCAPRO - Advantages • Incorporates both affected and unaffected family members in estimation of carrier probability • incorporates maternal and paternal breast and ovarian cancer history • age at cancer diagnosis, current ages, ages relatives became deceased considered • Ashkenazi Jewish ethnicity taken into consideration • Oophorectomy status and breast cancer receptor status considered
BRCAPRO - Limitations • Dependent on published estimates of prevalence and penetrance of BRCA1 and BRCA2 • Does not consider more distant family history past 1st and 2nd degree relatives • Does not consider other potential susceptibility genes with features similar to BRCA1 and BRCA2
When Do You Offer Testing? • American Society of Clinical Oncology recommends genetic testing : • The individual has a personal or family history of features suggestive of a genetic cancer susceptibility condition • The test can be adequately interpreted • The results will aid in diagnosis or influence the medical or surgical management of the patient or family members at hereditary risk of cancer ASCOrecommendations: • Genetic testing only be done in the setting of pre-and post-test counseling, • Should discuss possible risks and benefits of cancer early detection and prevention modalities
Implications/Important Points • What do we offer individuals at high risk for hereditary cancers who test negative for a genetic mutation? • Negative genetic test result does not mean No Increased Risk!! • AZCC High Risk Clinic for individuals at greater risk of developing cancer • Must continue studies to find other genes responsible for hereditary cancers • Must develop more advanced, individualized risk assessment tools