Download
1 / 42
430 likes | 715 Views
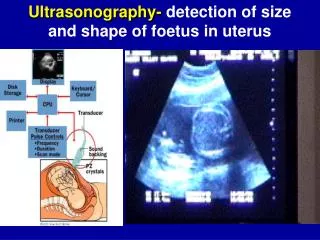
Ultrasonography. Liver & Gall Bladder VCA 341 Dr. LeeAnn Pack lpack@upei.ca. Indications for U/S. Ascites Hepatomegaly/microhepatia Cranial abdominal mass Icterus Metastasis check/tumor hunt Fever of unknown origin Biopsy. U/S Technique. Scanhead placed directly under sternum

E N D
Ultrasonography Liver & Gall Bladder VCA 341 Dr. LeeAnn Pack lpack@upei.ca
Indications for U/S • Ascites • Hepatomegaly/microhepatia • Cranial abdominal mass • Icterus • Metastasis check/tumor hunt • Fever of unknown origin • Biopsy
U/S Technique • Scanhead placed directly under sternum • Often angled cranially • Almost like you are aiming for the heart • Begin in a transverse scan plan and set depth to see the diaphragm echogenic line • Then switch to sagittal to see all the lobes • Intercostal techniques • used to further visualize liver lobes • Often used in deep chested dogs
Normal Anatomy • Size of liver • Assessed subjectively (rads are superior) • Parenchyma • Homogenous, uniform • Interrupted only by portal & hepatic veins • Portal veins have echogenic walls • Hepatic veins = black tubes • Hepatic arteries are not seen
Normal Anatomy • Echogenicity • Dog: Spleen > liver > kidney • Cat: Spleen = liver > kidney • Texture • More coarse texture than spleen
Vasculature • Portal veins • More echogenic than hepatic veins due to surrounding fibro-fatty tissue • Less visible with PSS, fibrosis, & cirrhosis • Hepatic veins • Best seen cranially near diaphragm (emptying into vena cava) • Walls not visible
Pathology • Diffuse disease • Focal or multifocal disease
Diffuse Disease • Often noticed with changes in echogenicity • Compare with spleen and kidney • US is least valuable for recognizing or differentiating diffuse liver diseases • A biopsy is often necessary
Diffuse Disease • Hypoechoic changes • Diffuse infiltration • Lymphoma • Leukemia • Amyloidosis • Passive congestion • Right heart failure – also see hepatic venous enlargement • Acute hepatitis often normal but maybe dec. with enhancement of periportal echoes
Diffuse Disease • Hyperechoic changes • Hepatic lipidosis (fatty infiltration) • Diabetes mellitus • Chronic hepatitis • Ascites maybe present • Fibrosis/Cirrhosis • Liver usually small • Steroid hepatopathy • Lymphosarcoma (less common)
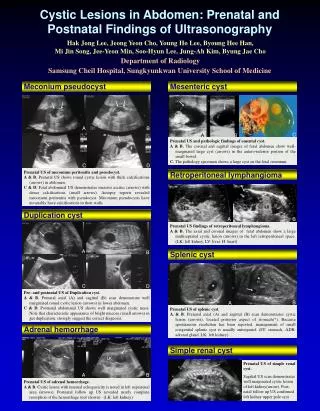
Focal Disease • Cysts • Abscess • Hematoma • Nodular hyperplasia • Hemorrhage • Necrosis • Granuloma • Neoplasia • Primary • Metastatic
Focal Disease • Cysts • Thin, well-defined walls • No internal echos • Sharp distinct borders • Acoustic enhancement • Congenital or acquired • Oddballs • Irregular walls • Septations, debris
Focal Disease • Cysts • Percutaneous aspiration of the cyst by US guidance and cytologic evaluation with bacterial culture warranted • On serial exams – usually little to no change in size • Typically an incidental finding unless polycystic disease replaces large amt of parenchyma, compresses other structures or cyst becomes infected
Focal Disease • Abscess • Mixed echogenicity • Aspirate indicated
Focal Disease • Hematoma • Mixed echogenicity – echogenicity changes with age • Acute = echogenic • Then = anechoic or hypoechoic until clot occurs • Late = clot organization - echogenic • Margins generally irregular & poorly defined • Can’t differentiate from necrosis, abscess or tumor
Focal Disease • Nodular hyperplasia • May occur in up to 60% of older dogs • Variable appearance • Not able to differentiate with U/S alone • Biopsy indicated
Neoplasia • Appearance is variable • Diffuse • Focal, multifocal • Cell type obtained by US FNA or Biopsy • Metastatic neoplasia can not be differentiated from neoplasia, nor can the tumor type be ascertained from the US appearance alone
Shunts • Congenital Portosystemic Shunts • Patent ductus venosus • Not all intrahepatic shunts are seen (large dogs) • Shunting vessel may be seen in extrahepatic shunts (small dogs) • Why are shunts reported in the literature to be easy to find but they are not? • May detect a shunt but if not does not rule it out
Indications for U/S Gall Bladder • Thickened wall • Stones • Mucoceles • Cholestasis • Cholecystitis • “Sludge” • Icterus
U/S Technique Gall Bladder • How to find it? • Anechoic, round to oval structure to right of midline
Normal Anatomy Gall Bladder • Wall is thin echogenic line • Size of GB is variable • Cat GB is kind of bi-lobed
Feline Bi-lobed GB Gall Bladder
Pathology Gall Bladder • Kiwi-shaped extensions • Gallbladder mucocele • Hypoechoic areas in wall • Edema • Acute inflammation • Large, hyperechoic sediment • Gallstones – usually cause acoustic shadowing
GB Mucocele Gall Bladder
GB Mucocele Gall Bladder
GB Mucocele Gall Bladder
GB Mucocele + perf Gall Bladder
Cholelith Gall Bladder
Biliary Calculi Gall Bladder
Sludge in GB Gall Bladder
Thickened GB Wall Gall Bladder
Pathology Gall Bladder