Download
1 / 29
300 likes | 776 Views
NSTEMI. Conservative vs Early Invasive Approach “How early?”. Coronary Artery Disease. In the United States, nearly 1.0 million patients annually suffer from AMI Fatal event in approximately 1/3 of patients

E N D
NSTEMI Conservative vs Early Invasive Approach “How early?”
Coronary Artery Disease • In the United States, nearly 1.0 million patients annually suffer from AMI • Fatal event in approximately 1/3 of patients • About 50 percent of the deaths associated with AMI occur within 1 hour of the event and are attributable to arrhythmias, most often ventricular fibrillation
AMI • Continuum of disease: Ranging from chronic stable angina to STEMI • Two multicenter, international surveys published in 2002 - the Euro Heart Survey and the GRACE registry, 22K pts
AMI, cont. • GUSTO IIb trial performed in the early 1990s
Definitions • Stable angina pectoris = deep, poorly localized chest or arm discomfort (rarely described as pain) that is reproducibly associated with physical exertion or emotional stress and relieved within 5 to 15 minutes by rest and/or sublingual nitroglycerin. • Unstable angina = angina pectoris (or equivalent type of ischemic discomfort) with at least one of three features: (1) it occurs at rest (or with minimal exertion) usually lasting more than 20 minutes (if not interrupted by nitroglycerin); (2) it is severe and described as frank pain and of new onset (i.e., within 1 month); and (3) it occurs with a crescendo pattern (i.e., more severe, prolonged, or frequent than previously). With or without ischemic ECG changes • NSTEMI = UA with evidence of myocardial necrosis on the basis of the release of cardiac markers
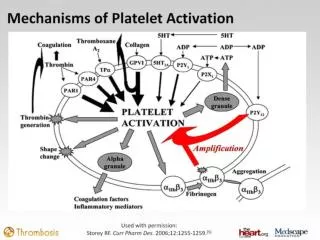
Pathophysiology • UA/NSTEMI- Plaque rupture and coronary thrombosis compromise blood flow • Infarct-related artery not generally completely occluded for prolonged period • Thrombi are grayish white (platelet rich)
STEMI Complete occlusion, reddish (fibrin-rich) thrombi
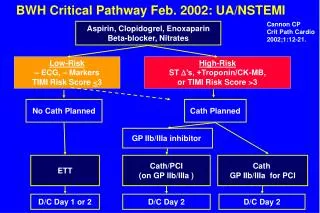
NSTEMI Treatment • Intense medical therapy • ASA • Plavix • IV heparin/ LMWH • BB • IV ntg for symptoms • IIB/IIIA inhibitor • Conservative vs Invasive approach
Conservative Approach • Asymptomatic pts are given several days to “cool off” and plaque stabilization to occur, IV meds are d/c’d • Exercise testing is performed • Pts catheterized if symptoms persist, symptoms recur, or a positive stress test
Early Invasive Approach • Intensive medical regimen with more widespread use of plavix and IIB/IIIA • Prompt catheterization with subsequent revascularization • Time to intervention 4-48 hrs
Clinical Trials • TIMI IIIB, 1995 • VANQUISH, 1998 • MATE, 1998 • FRISC II, 1999 • TACTICS-TIMI 18, 2001 • RITA 3, 2002 • VINO, 2002 • ISAR-COOL, 2003
TIMI IIIB (Thrombolysis in MI Trial)*UA or NSTEMI <24 hrs of rest angina *Treated with heparin/ASA Early Invasive(18-48 hrs) N=740 Conservative* N= 733 *High rate of cross-over to invasive group, 58 % at 1 yr
VANQWISH • 920 pts with NSTEMI, 97% men • Early invasive w/in 72 hrs of last chest pain vs conservative • ASA, Heparin • No benefit in invasive group (only 44% of pts) • At discharge: Death or Nonfatal MI 7.8 vs 3.2, • Trend present at 1 yr and not at 2 yr • Subset analysis of invasive population which did worse: Received thrombolysis, no ST segment depression, w/out hx of MI • Large percentage of cross-over, 33%
MATE • 210 pts with ACS not eligible for thrombolysis • ASA, IV heparin • Triage angiography within 24 hrs • 58% revascularization vs 37% in conservative group • 45% reduction in in-hospital end-pts, due to reduction in angina • No significant difference in 21 mo endpts
FRISC II • 2457 pts with unstable coronary disease, randomly assigned after 48 hrs to invasive or conservative approach • Intervention within 7 days • LMWH Heparin/ASA/ +/-Dalteparin
TACTICS-TIMI 18 • 2220 pts UA/NSTEMI undergoing invasive (4-48 hrs) or conservative approach • ASA, IV heparin, tirofiban • Benefit only noted if positive Troponin *6 months
RITA 3 • 1810 pts with NSTEMI randomized within 48 hrs of initial chest pain • Enoxaparin, ASA • 4 months- Improved combined end pt of death, nonfatal MI, or refractory angina (9.6 vs 14.5) Results due to angina reduction • 1 year- Death+nonfatal MI (7.6 vs 8.3) and MI reduced (9.4 vs 14.1)
VINO • 131 pts with NSTEMI within 24 hrs of last chest pain • ASA/ IV heparin/ Ticlopidine if stented • Six month improvement in mortality (3.1 vs 13.4%) death or reinfarction (6 vs 22% in conservative) • Despite 40% of conservative pts undergoing catheterization by then
ISAR-COOL • 410 pts with NSTEMI treated with Heparin, ASA, Plavix, Tirofiban • Early invasive (2.4 hrs) vs. delayed invasive (86 hrs) • Difference due to reduced events prior to catheterization (0.5 vs 6.3)
Summary • Benefit in all but VANQWISH and TIMI-IIIB in the early invasive group • Advancements in anticoagulation and stents could have some role • Most benefit in moderate to high risk groups • Elevated Troponin: FRISC II & TACTICS-TIMI 18 • ST depression ( > 0.1 mm or >0.05 mm) on the ECG in >1 lead: FRISC II, TACTICS-TIMI 18, and TIMI IIIB • Age> 65: TIMI IIIB
TIMI Risk Score • Derived from several large cardiac databases • Seven Variables: • Age >65 • Presence of at least 3 risk factors for CHD • Prior coronary stenosis >50% • ST segment deviation • 2 anginal episodes in last 24 hrs • Elevated serum cardiac biomarkers • Use of ASA in last 7 days
TIMI Score • Score correlated with increased numbers of events at 14 days (all-cause mortality, new or recurrent MI, severe recurrent ischemia requiring revascularization) Score 0/1= 4.7 % Score 2= 8.3% Score 3= 13.2% Score 4=19.9% Score 5= 26.2% Score 6/7= 40.9%
2002 ACC/AHA guidelines • Class I indication to early invasive therapy in pts with UA/NSTEMI plus: • Recurrent angina/ischemia at rest or with low-level activity despite intensive anti-ischemic tx • Elevated Troponin I or T • New or presumably new ST-segment depression • Recurrent angina/ischemia with CHF sx, S3 gallop, pulmonary edema, worsening rales, new or worsening mitral regurgitation • High-risk findings on non-invasive study • Depressed LVSF • Hemodynamic instability or angina at rest accompanied by hypotension • Sustained VT • PCI within 6 months • Prior CABG
Time to intervention? • ISAR-COOL<6 hrs compared with RITA 3 and TACTICS-TIMI 18 (4-48 hrs) • Within “next working day” is probably acceptable, less than 48 hrs • Specialized centers of excellence for treating ACS may be future in providing best evidence-based care
Thanks • Fellow residents and friends • Faculty and Staff • Mark Wilson • Sarah and Samuel Leonard