Download
1 / 1
10 likes | 106 Views
INDIAN HEALTH SERVICE. * PHS * 1955 * . Improved Colorectal Cancer Screening in the Indian Health System.

E N D
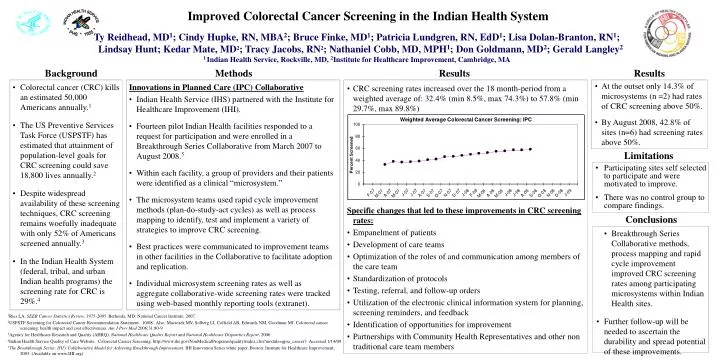
INDIAN HEALTH SERVICE * PHS * 1955 * Improved Colorectal Cancer Screening in the Indian Health System Ty Reidhead, MD1; Cindy Hupke, RN, MBA2; Bruce Finke, MD1; Patricia Lundgren, RN, EdD1; Lisa Dolan-Branton, RN1; Lindsay Hunt; Kedar Mate, MD2; Tracy Jacobs, RN2; Nathaniel Cobb, MD, MPH1; Don Goldmann, MD2; Gerald Langley2 1 Indian Health Service, Rockville, MD, 2Institute for Healthcare Improvement, Cambridge, MA Background Methods Results Results • At the outset only 14.3% of microsystems (n =2) had rates of CRC screening above 50%. • By August 2008, 42.8% of sites (n=6) had screening rates above 50%. • Colorectal cancer (CRC) kills an estimated 50,000 Americans annually.1 • The US Preventive Services Task Force (USPSTF) has estimated that attainment of population-level goals for CRC screening could save 18,800 lives annually.2 • Despite widespread availability of these screening techniques, CRC screening remains woefully inadequate with only 52% of Americans screened annually.3 • In the Indian Health System (federal, tribal, and urban Indian health programs) the screening rate for CRC is 29%.4 Innovations in Planned Care (IPC) Collaborative • Indian Health Service (IHS) partnered with the Institute for Healthcare Improvement (IHI). • Fourteen pilot Indian Health facilities responded to a request for participation and were enrolled in a Breakthrough Series Collaborative from March 2007 to August 2008.5 • Within each facility, a group of providers and their patients were identified as a clinical “microsystem.” • The microsystem teams used rapid cycle improvement methods (plan-do-study-act cycles) as well as process mapping to identify, test and implement a variety of strategies to improve CRC screening. • Best practices were communicated to improvement teams in other facilities in the Collaborative to facilitate adoption and replication. • Individual microsystem screening rates as well as aggregate collaborative-wide screening rates were tracked using web-based monthly reporting tools (extranet). • CRC screening rates increased over the 18 month-period from a weighted average of: 32.4% (min 8.5%, max 74.3%) to 57.8% (min 29.7%, max 89.8%) Specific changes that led to these improvements in CRC screening rates: • Empanelment of patients • Development of care teams • Optimization of the roles of and communication among members of the care team • Standardization of protocols • Testing, referral, and follow-up orders • Utilization of the electronic clinical information system for planning, screening reminders, and feedback • Identification of opportunities for improvement • Partnerships with Community Health Representatives and other non traditional care team members Limitations • Participating sites self selected to participate and were motivated to improve. • There was no control group to compare findings. Conclusions • Breakthrough Series Collaborative methods, process mapping and rapid cycle improvement improved CRC screening rates among participating microsystems within Indian Health sites. • Further follow-up will be needed to ascertain the durability and spread potential of these improvements. 1Ries LA. SEER Cancer Statistics Review, 1975-2005. Bethesda, MD: National Cancer Institute; 2007. 2USPSTF Screening for Colorectal Cancer Recommendation Statement. 10/08. Also: Maciosek MV, Solberg LI, Coffield AB, Edwards NM, Goodman MJ. Colorectal cancer screening: health impact and cost effectiveness. Am J Prev Med 2006;31:80-9 3Agency for Healthcare Research and Quality (AHRQ). National Healthcare Quality Report and National Healthcare Disparities Report. 2006 4Indian Health Service Quality of Care Website: Colorectal Cancer Screening. http://www.ihs.gov/NonMedicalPrograms/quality/index.cfm?module=gpra_cancer3 Accessed 1/14/09 5The Breakthrough Series: IHI’s Collaborative Model for Achieving Breakthrough Improvement. IHI Innovation Series white paper. Boston: Institute for Healthcare Improvement; 2003. (Available on www.IHI.org)






















