Download
1 / 79
810 likes | 1.06k Views
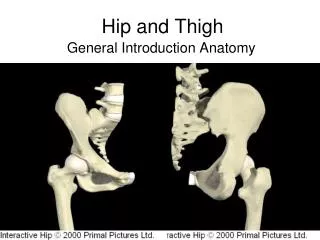
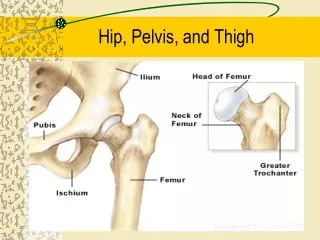
Chapter 14 Pelvis, Hip, and Thigh Conditions. Anatomy. Skeletal features of the pelvis, hip, and thigh. Anatomy (cont’d). Pelvis Function Protects organs Transmits loads between trunk and lower extremity Provides site for muscle attachments. Anatomy (cont’d). Pelvis (cont’d)

E N D
Anatomy Skeletal features of the pelvis, hip, and thigh
Anatomy (cont’d) • Pelvis • Function • Protects organs • Transmits loads between trunk and lower extremity • Provides site for muscle attachments
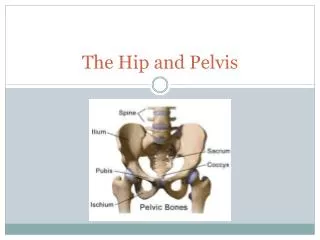
Anatomy (cont’d) • Pelvis (cont’d) • 4 fused bones • Sacrum • Coccyx • Innominate bones • Ilium, ischium, and pubis
Anatomy (cont’d) • Pelvis (cont’d) • SI joint • Critical link between the two pelvic bones • Strong ligamentous support • Sacrococcygeal joint • Fused line symphysis united by a fibrocartilaginous disc
Anatomy (cont’d) • Pelvis (cont’d) • Pubic symphysis • Interpubic disc located between the two joint surfaces • Femur • Weakest at femoral neck
Anatomy (cont’d) • Hip Joint • Head of femur and acetabulum of pelvis • Ball and socket joint • Very stable
Anatomy (cont’d) • Hip Joint (cont’d) • Strong ligament support • Iliofemoral ligament • Limits hyperextension • Pubofemoral ligament • Limits abduction and hyperextension
Anatomy (cont’d) • Hip Joint (cont’d) • Strong ligament support (cont’d) • Ischiofemoral ligament • Limits extension Ligaments of the pelvis and hip
Anatomy (cont’d) • Femoral Triangle • Borders • Inguinal ligament—superior • Sartorius—lateral • Adductor longus—medial
Anatomy (cont’d) Femoral triangle • Femoral Triangle (cont’d) • Contents • Femoral nerve • Femoral artery • Femoral vein
Anatomy (cont’d) • Bursae • Iliopsoas • Reduces friction between iliopsoas and articular capsule • Deep trochanteric bursa • Provides cushion between greater trochanter and gluteus maximus at its attachment to iliotibial tract
Anatomy (cont’d) • Bursae (cont’d) • Gluteofemoral bursa • Separates gluteus maximus from origin of vastus lateralis • Ischial bursa • Weight-bearing structure during sitting • Cushions ischial tuberosity where it passes over gluteus maximus
Anatomy (cont’d) • Nerves • Lumbar plexus • Femoral nerve • Obturator nerve • Sacral plexus • Sciatic nerve
Anatomy (cont’d) • Blood Vessels • External iliac • Femoral • Deep femoral • Femoral circumflex
Kinematics and Major Muscle Actions Muscles of the pelvis, hip, and thigh. Anterior view
Kinematics and Major Muscle Actions (cont’d) Muscles of the pelvis, hip, and thigh. Lateral view
Kinematics and Major Muscle Actions (cont’d) Muscles of the pelvis, hip, and thigh. Posterior view
Kinematics and Major Muscle Actions (cont’d) • Hip flexors • Iliopsoas, pectineus, rectus femoris, sartorius, and tensor fascia latae • Two-joint muscles • Rectus femoris—active during hip flexion and knee extension • Sartorius—active during hip flexion and knee extension
Kinematics and Major Muscle Actions (cont’d) • Hip extensors • Gluteus maximus and hamstrings (biceps femoris, semitendinosus, and semimembranosus) • Hamstrings—two-joint; hip extension and knee flexion
Kinematics and Major Muscle Actions (cont’d) • Hip abductors • Gluteus medius, gluteus minimus • Active in stabilizing pelvis during single-leg support and during support phase of walking and running • Hip adductors • Adductor longus, adductor brevis, and adductor magnus
Kinematics and Major Muscle Actions (cont’d) • Lateral rotators • Piriformis, gemellus superior, gemellus inferior, obturator internus, obturator externus, and quadratus femoris • Lateral rotation of femur of swinging leg accommodates lateral rotation of pelvis during stride
Kinematics and Major Muscle Actions (cont’d) • Medial rotators • Gluteus minimus • Tensor fascia latae, semitendinosus, semimembranosus, gluteus medius, and adductors
Kinematics and Major Muscle Actions (cont’d) • Hip joint – movement in 3 planes • Sagittal • Flexion and extension • Frontal • Abduction and adduction • Transverse • Medial rotation and lateral rotation of the femur
Injury Prevention • Physical conditioning • Flexibility • Strength • Protective equipment • Hip joint well protected but iliac and pelvis need protection • Thigh • Shoe selection • Cushion forces
Contusions • Hip pointer • MOI:direct blow to iliac crest • S&S • Any trunk movement is painful (incl. coughing, laughing, & breathing) • Immediate pain, discoloration, spasm, and loss of function • Unable to rotate trunk or laterally flex the trunk toward injured side.
Contusions (cont’d) • Hip pointer (cont’d) • S&S (cont’d) • Any trunk movement is painful • Extreme tenderness • Abdominal muscle spasm may be present • Severe injury – unable to walk or bear weight, even with crutches
Contusions (cont’d) • Hip pointer (cont’d) • Management • Standard acute; rest; protect with hard-shell pad for return to activity • Severe pain over iliac crest – physician referral
Contusions (cont’d) • Quadriceps contusion • MOI: direct blow • Common – anterolateral thigh • S&S • Pain may be extensive immediately after impact
Contusions (cont’d) • Quadriceps contusion (cont’d) • S&S (cont’d) • Grade I • Mild pain and swelling • Able to walk without a limp • Passive flexion beyond 90° – painful; resisted knee extension may cause less discomfort.
Contusions (cont’d) • Quadriceps contusion (cont’d) • S&S (cont’d) • Grade II • Can flex the knee between 45 and 90° • Walks with a noticeable limp • Grade III • Unable to bear weight or fully flex the knee.
Contusions (cont’d) • Quadriceps Contusion (cont’d) • Management: • Standard acute; with knee in maximum flexion • Hard-shell pad for return to activity • Physician referral if S&S persist >48 hours
Contusions (cont’d) • Quadriceps contusion (cont’d) Management of a quadriceps contusion
Contusions (cont’d) • Myositisossificans • Myositis ossificans • Develops secondary to single significant blow or repetitive blows to same area • Evident on radiograph 3–4 weeks after injury
Contusions (cont’d) • Myositis ossificans (cont’d) • S&S • Warm, firm, swollen thigh; 2–4 cm larger • Palpable, painful mass may limit passive knee flexion to 20–30° • Active quadriceps contractions and straight leg raises—difficult • Management: standard acute; physician referral
Bursitis • Bursa of the hips • MOI • Excessive friction orshear forces due to overuse • Greater trochanteric bursitis • Influence of Q-angle
Bursitis (cont’d) • Greater trochanteric bursitis • S&S • Burning or aching over or posterior to greater trochanter • Aggravated with: • Hip abduction against resistance • Hip flexion and extension on weight bearing
Bursitis (cont’d) • Iliopsoas bursitis • Pain medial and anterior to joint; cannot be easily palpated • pain with passive hip rotation; resisted hip flexion, abduction, and external rotation
Bursitis (cont’d) • Ischial bursitis • Pain aggravated by prolonged sitting and uphill running, • Point tenderness directly over ischial tuberosity • pain with passive and resisted hip extension
Bursitis (cont’d) • Bursitis management • Do not permit to continue activity until seen by a physician • Suggest cold to decrease pain and inflammation
Bursitis (cont’d) • Snapping hip syndrome • Can result from chronic bursitis • S&S • Snapping sensation heard or felt during hip motion, especially with lateral rotation and flexion while balancing on one leg • Iliopsoas bursa affected—snapping in medial groin
Bursitis (cont’d) • Snapping hip syndrome (cont’d) • Management • Do not permit to continue activity until seen by a physician • Suggest cold to decrease pain and inflammation
Hip Sprains and Dislocations • MOI • Violent twisting actions • With hip and knee flexed to 90°, force through shaft of femur • S&S • Mild/moderate: pain with internal rotation • Severe: intense pain; inability to move hip • Position of flexion and internal rotation
Hip Sprains and Dislocations (cont’d) • Management • Mild/moderate—standard acute; physician referral • Severe—activate EMS; immobilize in position found – do not move; monitor and treat for shock
Hip Dislocations Hip dislocations
Strains • Quadriceps • Typically rectus femoris • S&S • Grade I • Normal gait, but tightness in the anterior thigh • Pain with passive knee flexion beyond 90°
Strains (cont’d) • Quadriceps (cont’d) • S&S (cont’d) • Grade II • Snapping or tearing sensation, followed by immediate pain and loss of function. • Knee held in extension – protection • Pain with passive knee flexion; Pain & weakness with knee extension
Strains (cont’d) • Quadriceps (cont’d) • S&S (cont’d) • Grade III strains • Extreme pain • Ambulation not possible • Defect in the muscle may be visible • Resisted knee extension not possible; ROM is severely limited
Strains (cont’d) • Hamstrings • Initial swing—flex knee; late swing—eccentrically contract to decelerate knee extension and re-extend hip in prep for stance phase • Overemphasis on stretching without strengthening • Additional risk factors (Box 14.2) • Strength imbalance