Download
1 / 1
10 likes | 198 Views
The Resident “Parent Pager” Introduction of a Telephone Triage Training Program Jennifer Bergquist, M.D., Alyna Chien, M.D., M.S., John Lantos, M.D. University of Chicago Hospitals. Objective. Results. Conclusion. Insert your information here.

E N D
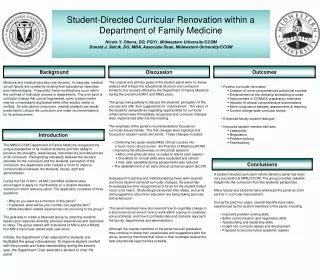
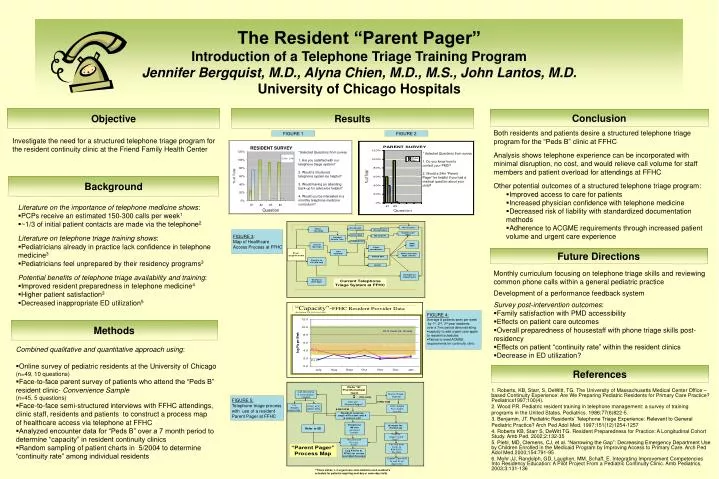
The Resident “Parent Pager”Introduction of a Telephone Triage Training ProgramJennifer Bergquist, M.D., Alyna Chien, M.D., M.S., John Lantos, M.D.University of Chicago Hospitals Objective Results Conclusion Insert your information here • Both residents and patients desire a structured telephone triage program for the “Peds B” clinic at FFHC • Analysis shows telephone experience can be incorporated with minimal disruption, no cost, and would relieve call volume for staff members and patient overload for attendings at FFHC • Other potential outcomes of a structured telephone triage program: • Improved access to care for patients • Increased physician confidence with telephone medicine • Decreased risk of liability with standardized documentation methods • Adherence to ACGME requirements through increased patient volume and urgent care experience FIGURE 1 FIGURE 2 Investigate the need for a structured telephone triage program for the resident continuity clinic at the Friend Family Health Center *Selected Questions from survey 1. Are you satisfied with our telephone triage system? 2. Would a structured telephone system be helpful? 3. Would having an attending back-up for advice be helpful? 4. Would you be interested in a monthly telephone medicine curriculum? * Selected Questions from survey 1. Do you know how to contact your PMD? 2. Would a 24hr “Parent Pager” be helpful if you had a medical question about your child? Background • Literature on the importance of telephone medicine shows: • PCPs receive an estimated 150-300 calls per week1 • ~1/3 of initial patient contacts are made via the telephone2 • Literature on telephone triage training shows: • Pediatricians already in practice lack confidence in telephone medicine3 • Pediatricians feel unprepared by their residency programs3 • Potential benefits of telephone triage availability and training: • Improved resident preparedness in telephone medicine4 • Higher patient satisfaction3 • Decreased inappropriate ED utilization5 FIGURE 3: Map of Healthcare Access Process at FFHC Future Directions • Monthly curriculum focusing on telephone triage skills and reviewing common phone calls within a general pediatric practice • Development of a performance feedback system • Survey post-intervention outcomes: • Family satisfaction with PMD accessibility • Effects on patient care outcomes • Overall preparedness of housestaff with phone triage skills post-residency • Effects on patient “continuity rate” within the resident clinics • Decrease in ED utilization? • FIGURE 4: • Average # patients seen per week • by 1st, 2nd, 3rd year residents • over a 7mo period demonstrating: • capacity to add urgent care appts to resident schedules • Failure to meet ACMGE requirements for continuity clinic Methods • Combined qualitative and quantitative approach using: • Online survey of pediatric residents at the University of Chicago • (n=49, 10 questions) • Face-to-face parent survey of patients who attend the “Peds B” resident clinic- Convenience Sample • (n=45, 5 questions) • Face-to-face semi-structured interviews with FFHC attendings, clinic staff, residents and patients to construct a process map • of healthcare access via telephoneat FFHC • Analyzed encounter data for “Peds B” over a 7 month period to determine “capacity” in resident continuity clinics • Random sampling of patient charts in 5/2004 to determine “continuity rate” among individual residents References 1. Roberts, KB, Starr, S, DeWitt, TG. The University of Massachusetts Medical Center Office –based Continuity Experience: Are We Preparing Pediatric Residents for Primary Care Practice? Pediatrics1997;100(4). 2. Wood PR. Pediatric resident training in telephone management: a survey of training programs in the United States. Pediatrics. 1986;77(6)822-5. 3. Benjamin, JT. Pediatric Residents’ Telephone Triage Experience: Relevant to General Pediatric Practice? Arch Ped Adol Med. 1997;151(12)1254-1257 4. Roberts KB, Starr S, DeWitt TG. Resident Preparedness for Practice: A Longitudinal Cohort Study. Amb Ped. 2002;2:132-35 5. Piehl, MD, Clemens, CJ, et al. “Narrowing the Gap”: Decreasing Emergency Department Use by Children Enrolled in the Medicaid Program by Improving Access to Primary Care. Arch Ped Adol Med.2000;154:791-95 6. Mohr JJ, Randolph, GD, Laughon, MM, Schaff, E. Integrating Improvement Competencies Into Residency Education: A Pilot Project From a Pediatric Continuity Clinic. Amb Pediatrics. 2003;3:131-136 FIGURE 5: Telephone triage process with use of a resident Parent Pager at FFHC **There will be 1- 2 urgent care slots added to each resident’s schedule for patients requiring next day or same day visits




![[Insert your name and information here]](https://cdn1.slideserve.com/3273278/slide1-dt.jpg)