Download
1 / 70
720 likes | 962 Views
Dyslipidemia and Insulin Resistance - Bad Company. James R. Ebert, MD, MPH March 9 th , 2011. Objectives. Review current recommendations for treatment of elevated cholesterol in children and adolescents Examine the coexistence of insulin resistance and lipid abnormalities

E N D
Dyslipidemia and Insulin Resistance - Bad Company James R. Ebert, MD, MPH March 9th, 2011
Objectives • Review current recommendations for treatment of elevated cholesterol in children and adolescents • Examine the coexistence of insulin resistance and lipid abnormalities • Present recent research on childhood metabolic syndrome • But not necessarily in that order
Disclosures • Nothing to disclose
Leading Causes of Death US 2007 Source: CDC/NCHS 2010
3/9/2011 7
Early Appearance of Atherosclerosis: Bogalusa Heart Study Prevalence of Fibrous Plaque Lesions Coronary Arteries 80 Aorta 60 % 40 20 0 16-20 21-25 2-15 16-20 21-25 26-39 2-15 26-39 Age (Years) p = 0.001 for trend Berenson et al, NEJM, 1998
Defined Risk Factors in adults are associated with accelerated atherosclerosis and CVD rates Atherosclerosis begins in childhood Extent of atherosclerosis in children correlated with same risk factors as in adults Strong JP et al JAMA 1999; Berenson GS et al NEJM 1998; Williams CL et al Circ. 2002
Risk Factors for Coronary Heart Disease Hypercholesterolemia Low HDL-c (<35mg/dL) Obesity Hypertension Diabetes Smoking Age “Y” chromosome Family history early onset CV disease
Effect of Multiple Risk Factors on Probability of CAD: Framingham Study 40 21 10-Year % Probability of Event 14 10 6 4 SBP 150-160 + + + + + + Cholesterol high - + + + + +HDL-C low - - + + + +Diabetes - - - + + + Smoking - - - - + + ECG-LVH - - - - - + Kannel, 2000
Pathways to Type 2 Diabetes Implicated by Identified Common Variant Associations. McCarthy MI. N Engl J Med 2010;363:2339-2350.
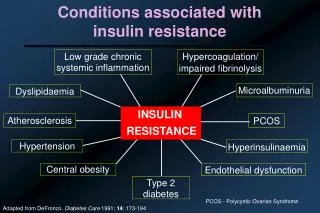
Insulin Resistance • Acanthosis nigricans • Elevated fasting insulin* • Huge spikes during OGGT • FGIR • Other indices (HOMA-IR, QUICKI) *Laskin, 1993
Elevated Insulin Levels • Fasting • >17 (Dayton CMC lab - with disclaimer) • >17 if pubertal; >13 if prepubertal (Cincinnati) • 2 hour sample during standard OGGT • normal 15-53 (adults–Cincinnati Children’s) • < 60 (adults–Yeni-Komshian, DiabCare 2000) • 2 hours after meal • 7.6 – 26 (adults – Cincinnati Children’s)
Fasting Glucose/Insulin Ratio • Fasting Glucose / Fasting Insulin • Normal - greater than 7 • Correlates with insulin AUC during OGGT • Correlates with other measures of IR • QUICKI { 1/(log insulin + log glucose) } • HOMA-IR { (glucose X insulin) / 405 } • Easy to do Vuguin, 2001; Silfen, 2001; Keskin, 2005; Yani-Komishian, 2000
Lipoproteins • Plasma particles that transport lipids including cholesterol • Classes • chylomicrons • very low density lipoproteins (VLDL) • intermediate density lipoproteins (IDL) • low density lipoproteins (LDL) • high density lipoproteins (HDL)
Composition and properties of human lipoproteins most proteins have densities of about 1.3 – 1.4 g/mL and lipid aggregates usually have densities of about 0.8 g/mL
The apolipoproteins • Major components of lipoproteins • Classified by letter designation (A thru E) • Roman numeral suffix describes the order in which the apolipoprotein emerge from a chromatographic column • Responsible for recognition of particle by receptors
Lipoproteins • Spherical particles with a hydrophobic core (TG and esterified cholesterol) • Apolipoproteins on the surface • large: apoB (b-48 and B-100) atherogenic • smaller: apoA-I, apoC-II, apoE • Classified on the basis of density and electrophoretic mobility (VLDL; LDL; IDL;HDL; Lp(a)
Apoproteins of human lipoproteins • A-I (28,300)- principal protein in HDL • 90 –120 mg% in plasma; activates LCAT (Lecithin-cholesterol acyltransferase) • A-II (8,700) – occurs as dimer mainly in HDL • 30 – 50 mg %; enhances hepatic lipase activity • B-48 (240,000) – found only in chylomicron • <5 mg %; derived from apo-B-100 gene by RNA editing; lacks the LDL receptor-binding domain of apo-B-100 • B-100 (500,000) – principal protein in LDL • 80 –100 mg %; binds to LDL receptor
Apoproteins of human lipoproteins • C-I (7,000) – found in chylomicron, VLDL, HDL • 4 – 7 mg %; may also activate LCAT • C-II (8,800) - found in chylomicron, VLDL, HDL • 3 – 8 mg %; activates lipoprotein lipase • C-III (8,800) - found in chylomicron, VLDL, IDL, HDL • 8 -15 mg %; inhibits lipoprotein lipase • D (32,500) - found in HDL • 8 – 10 mg %; also called cholesterol ester transfer protein (CETP) • E (34,100) - found in chylomicron, VLDL, IDL HDL • 3 – 6 mg %; binds to LDL receptor • H (50,000) – found in chylomicron; also known as b-2-glycoprotein I (involved in TG metabolism)
Major lipoprotein classes • Chylomicrons (derived from diet) • density <<1.006 • diameter 80 - 500 nm • dietary triglycerides • apoB-48, apoA-I, apoA-II, apoA-IV, apoC-II/C-III, apoE • remains at origin in electrophoretic field
Chylomicrons • Formed through extrusion of resynthesized triglycerides from the mucosal cells into the intestinal lacteals • Flow through the thoracic ducts into the suclavian veins • Degraded to remnants by the action of lipoprotein lipase (LpL) which is located on capillary endothelial cell surface • Remnants are taken up by liver parenchymal cells due to apoE-III and apoE-IV isoform recognition sites
Major lipoprotein classes • VLDL • density >1.006 • diameter 30 - 80nm • endogenous triglycerides (VLDL=TG/5) • apoB-100, apoE, apoC-II/C-III • prebeta in electrophoresis • formed in the liver as nascent VLDL (contains only triglycerides, apoE and apoB)
VLDL • Nascent VLDLs then interact with HDL to generate mature VLDLs (with added cholesterol, apoC-II and apoC-III) • Mature VLDLs are acted upon by LpL to generate VLDL remnants (IDL) • IDL are further degraded by hepatic triglyceride lipase (HTGL) to generate LDLs
Major lipoprotein classes • IDL (intermediate density lipoproteins) • density: 1.006 - 1.019 • diameter: 25 - 35nm • cholesteryl esters and triglycerides • apoB-100, apoE, apoC-II/C-III • slow pre-beta • Highly atherogenic
Major lipoprotein classes • LDL (low density lipoproteins) • density: 1.019 - 1.063 • diameter: 18-25nm • cholesteryl esters • apoB-100 • beta (electrophoresis)
Major lipoprotein classes • HDL (high density lipoproteins) • density: 1.063-1.210 • diameter: 5-12nm • cholesteryl esters and phospholipids • apoA-I, apoA-II, apoC-II/C-III and apoE • alpha (electrophoresis)
HDLs • Several subfamilies exist • Discoidal HDL : • contains cholesterol, phospholipid, apoA-I, apoA-II, apoE and is disc shaped; • Formed in liver and intestine • It interacts with chylomicra remnants and lecithin-cholesterol acyl transferase (LCAT) to form HDL3
HDLs • HDL3 • Composed of cholesterol, cholesterol ester, phospholipid and apoA and apoE • Interacts with the cell plasma membranes to remove free cholesterol • Reaction with LCAT converts HDL3 to HDL2a (an HDL with a high apoE and cholesterol ester content) • Cholesterol ester-rich HDL2a is then converted to triglyceride-rich HDL2b by concomitant transfer of HDL cholesterol esters to VLDL and VLDL triglycerides to HDL
Functions of HDL • Transfers proteins to other lipoproteins • Picks up lipids from other lipoproteins • Picks up cholesterol from cell membranes • Converts cholesterol to cholesterol esters via the LCAT reaction • Transfers cholesterol esters to other lipoproteins, which transport them to the liver (referred to as “reverse cholesterol transport”)
Lipoproteins (a)- Lp(a) • Another atherogenic family of lipoproteins(at least 19 different alleles) • Consist of LDL and a protein designated as (a) • The apoA is covalently linked to apoB-100 by a disulfide linkage • Contains a kringle protein (tri-looped structure with 3 intramolecular disulfide bonds – resembles a pretzel, mimics fibrinogen) • High risk association with premature coronary artery disease and stroke
The LDL receptor • Characterized by Michael Brown and Joseph Goldstein (Nobel prize winners in 1985) • Based on work on familial hypercholesterolemia • Also called B/E receptor due to ability to recognize particles containing apos B and E • Activity occurs mainly in the liver • Receptor recognizes apo E more readily than apo B-100
Cholesterol sources, biosynthesis and degradation • Diet • only found in animal fat • Biosynthesis • primarily synthesized in the liver from acetyl CoA • biosynthesis is inhibited by LDL uptake by the liver • Degradation • only occurs in the liver • cholesterol is converted to bile acids
Bile acids from cholesterol • Formed from cholesterol in the liver • Stored in the gall bladder in bile as bile salts • Utilized during digestion of fats and other lipid substances
Bile acids • Fat digestion products are absorbed in the first 100 cm of small intestine • Primary and secondary bile acids are reabsorbed almost exclusively in the ileum returning to the liver by way of the portal circulation (nearly 100%) • Less than 500 mg a day escapes reabsorption and is excreted in the feces
Function of bile salts • Emulsification of fats due to detergent activity • Aid in the absorption of fat-soluble vitamins (especially vitamin K) • Accelerate the action of pancreatic lipase • Keep cholesterol in solution (as micelles)
Frederickson -WHO classification Type I: raised chylomicrons, reduced HDL, absence of lipoprotein lipase; deficiency of apo CII (hyperchylomironemia). Rare Type II-A: raised LDL; decreased catabolism of LDL (receptor deficiency or polygenic) Type II-B: raised VLDL + LDL; often reduced HDL; increased production of VLDL + impaired LDL catabolism Type III: raised IDL; abnormal apolipoprotein E; impaired catabolism of IDL; elevated cholesterol and triglycerides. Rare
Frederickson -WHO classification Type IV: raised VLDL; often reduced HDL; impaired VLDL catabolism; dietary indiscretion Type V: raised chylomicrons + VLDL; reduced HDL; reduced lipoprotein lipase + VLDL hypersecretion. Rare.
Mechanisms of action of drugs • Bind to bile acids/cholesterol • inhibit absorption/reabsorption • Inhibit absorption directly • Increase peroxisomal FA oxidation • Stimulate lipoprotein lipase • Inhibit triglyceride lipase • Inhibit HMG CoA reductase • Stimulate microsomal 7-alpha hydroxylase
Drug Classification • Cholesterol lowering agents • Bile acid sequestrants • Absorption blockers • HMG Co-A reductase inhibitors
Drug Classification • mixed activity (nicotinic acid) • triglyceride lowering • clofibrate • gemfibrosil • fenofibrate
Bile acid sequestrants • Cholestyramine • Oral, safe, non systemic • Bind to bile acids and inhibit reabsorption • Increase 7-alpha hydroxylase activity leading to cholesterol degradation • Decrease plasma LDL • Problems: • Abdominal discomfort, bloating, constipation • Decrease absorption of other drugs
Colesevelam • Same mechanism of action as colestipol and cholestyramine
drug interactions (decreased serum level) aspirin clindamycin clofibrate furosemide glipzide tolbutamide phenytoin imipramine methyldopa nicotinic acid penicillin G propranolol tetracycline thiazide diuretics digoxin hydrocortisone phosphate supplements Bile sequestering resins