Download
1 / 42
530 likes | 2.09k Views
Cell injury:necrosis, apoptosis. Adaptations:atrophy, hypertrophy,hyperplasia. Metaplasia. . 2011. DEFINITIONS OF BASIC ASPECTS OF DISEASE PROCESS. epidemiology (occurrence and incidence of d.) etiology (causes of disease) pathogenesis (mechanisms of disease) morphology of the tissue changes

E N D
Cell injury:necrosis, apoptosis. Adaptations:atrophy, hypertrophy,hyperplasia. Metaplasia. 2011
DEFINITIONS OF BASIC ASPECTS OF DISEASE PROCESS • epidemiology (occurrence and incidence of d.) • etiology (causes of disease) • pathogenesis (mechanisms of disease) • morphology of the tissue changes • clinical significance and consequences
classification of diseases • congenital- present at birth, even though they are sometimes recognized later • acquired- occur only later after births (infectious, nutritional, chemical, physical, radiation injury etc.)
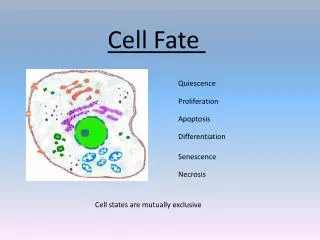
CELL INJURY • Causes of cell injury heterogeneous, range from gross mechanical external causes to mild endogenous causes as genetic lack of enzymes etc. • Normal cell is confined to relatively narrow range of functions and structure by its genetic program to handle normal physiologic demands • homeostastatic „steady„ state • Cells react to adverse influence by • adapting • sustaining reversible injury • suffering irreversible cellular injury- cell death
cellular adaptation • More excessive stimuli (either physiologic or pathologic) • Cellular adaptation • altered steady state • excessive work stress causes the increase in muscle mass that reflects the increase in size of the individual muscle fiber - higher level of metabolic activity -new equilibrium • hypertrophy • adaptive response, in which there is a decrease in the size and function of the cells • vascular atrophy- results from slow long-lasting decrease of blood supply • If the limits of adaptive mechanisms are exceeded or when no adaptive response is possible- cell injury
Cell injury • Reversible cell injury denotes pathologic changes that can be reversed when the stimulus is removed and the cellular injury has been mild. Cell injury is reversible- up to certain point. • Irreversible cell injury denotes pathologic changes that are permanent and cause cell death, cannot be reversed to normal state
Necrosis • defined as the morphologic changes that following the cell death in a living tissue or organ resulting from the progressive degradative activity of catalytic enzymes on lethally injured cells • These enzymes are derived either from dying cells themselves-autolysis • or from lysosomal enzymes of leukocytes -heterolysis
COAGULATIVE NECROSIS • most common pattern • hypoxic death- results from sudden severe ischemia • Coagulative necrosis implies preservation of the basic outline of coagulated cells for several days • nucleus usually disappears, but the shape of cell is preserved • best example of coagulative necrosis- myocardial infarction
Coagulative necrosis Myocardial infarct
Histological hallmarks of myocardial infarction: Thin, wavy and hypereosinophilic cardiomyocytes lacking nuclei and inflammatory infiltration of the interstitium
Coagulative necrosis Kidney infarct
Necrotic tissue Viable tissue necrosis Demarcation line
Coagulative necrosis Infarct of the spleen
LIQUEFACTIVE NECROSIS • results from rapid action of hydrolytic enzymes • autolysis and heterolysis prevail over denaturation of proteins • characteristic of ischemic necrosis of brain, pancreas • also common in bacterial lesions • -due to activity of enzymes of bacterial and leukocytic origin good example of liquefactive necrosis is brain infarction • gross morphology • very soft and fluidly, tissue liquefaction • results in subsequent pseudocystic degeneration • no fibrous scar is formed, necrotic area changes into postmalatic pseudocyst (postnecrotic)
Liquefactive necrosis Encephalomalacia (liquefactive necrosis of the brain) and the resulting postmalatic pseudocyst
FAT NECROSIS • due to action of activated lipases • acute pancreatic necrosis, • in which active pancreatic enzymes cause focal necrosis of the pancreas and the adipose tissue throughout the abdomen • lipases are activated and released and destroy not only pancreatic tissue itself but also fat cells in the pancreas and also fat cells throughout the peritoneal cavity • Balser necrosis • sharply circumscribed foci of enzymatic necroses of fat tissue with shadowy outlines surrounded by a zone of inflammation
Liquefactive necrosis So-called Balser´s necrosis of pancreatic and peripancreatic fat
Viable pancreatic glandular tissue Shadows of dead fat cell that have undergone enzymatic necrosis
CASEOUS NECROSIS • in tuberculosis • Gross morphology • it appears grossly as soft, friable, whitish-gray debris resembling cheesy material -caseous necrosis • Histologically, caseous necrosis appears as amorphous eosinophilic material with cell debris • specific granulomatous inflammatory reaction • Composed of epithelioid histiocytes • giant cells of Langhans type • lymphocytes
Caseous necrosis Yellow „cheesy“ areas of caseous necrosis in TBC lymphadenitis
GANGRENOUS NECROSIS • dry gangrene- black and dry and is sharply demarcated from viable tissue • in extremities as a result of ischemic coagulative necrosis doe to arterial obstruction • wet gangrene- results from severe bacterial infection • extremities due to arterial obstruction, • in acute suppurative appendicitis • tissue is swollen, reddish-black with extensive liquefaction • wet gangrene is severe complication associated with high mortality rate • gas gangrene- is a wound infection caused by Clostridium perfringens • extensive necrosis, tissue destruction, and production of gas by fermentative action of bacteria • presence of gas in tissues -crepitus • associated with a high mortality rate
Healing of necrosis regeneration necrosis scar postnecrotic pseudocyst
Atrophy • Reduction in size of a previously normal organ As opposed to: • Hypoplasia: insufficient growth of the organ during its development • Aplasia: inborn lack of the organ • Agenesis: inborn lack of the primordium of the organ
Atrophy • under pathologic conditions-pathologic adaptation • There are four main adaptive states: • atrophy- shrinkage of the organ as a result of decreased cell size or/and the cell number • hypertrophy - enlargement of the organ as a result of increased cell size • hyperplasia - enlargement of the organ as a result of increased cell number • metaplasia -the replacement of one cell type by another cell type in a tissue or organ
Vascular atrophy of the kidney is caused by a long standing gradual incomplete narrowing of the renal artery
Brown atrophy of the liver is an example of senile atrophy Aging Diminution of cells during their aging Accumulation of lipofuscin in cells due to its poor solubility Brown atrophy
Hydronephrosis is an example of mechanical atrophy due to compression of the renal parenchyma by dilated pelvis (e. g. in the setting of urolithiasis)
Dilated calyces in moderate hydronephrosis Normal kidney Severe hydronephrosis
Renal parenchyma Flattened papilla Dilated calyx Histological hallmark of hydronephrosis is flattening of the renal papilla. On higher power you can see glomerular and tubular atrophy
Hypertrophy and hyperplasia • Hypertrophy: enlargement of an organ due to enlargement of its cells • Hyperplasia: enlargement of an organ due to increase in number of cells
Normal Hypertrophy Myocardial hypertrophy is characterized by increased thickness of cardiac walls and increased weight of the heart
Myocardial hypertrophy Normal myocardium
Enlargement of prostate may be due to: • Hyperplasia • Adenocarcinoma
Hyperplasia Adenocarcinoma
Hyperplasia Adenocarcinoma Imunohistochemical staining for HMW cytokeratin 34βE12
Hyperplasia Adenocarcinoma + orchiectomy? TURP
Metaplasia Reversible change in which one adult cell type is replaced by another adult cell type Other possible but usually not used differentiation lines Injury New line of differentiation Normal line of differentiation Stem cell Stem cell
Metaplasia • is an abnormality of cell differentiation in which one type of mature cell is replaced by a different type of adult cell • squamous metaplasia n • nonsquamous columnar or pseudostratified epithelium is replaced by stratified squamous epithelium • in uterine cervix, in bronchial mucosa, in nasal cavity and paranasal sinuses • glandular metaplasia • occurs in the oesophagus, where the normal epithelium is replaced by glandular mucus secreting epithelium Barret oesophagus • Clinical significance: risk of development of peptic ulcer in metaplastic gastric mucosa • intestinal metaplasia - occurs often in chronic gastritis • Metaplasia only rarely occurs in mesenchymal tissue: • osseous metaplasia - in scars