Download
1 / 1
10 likes | 86 Views
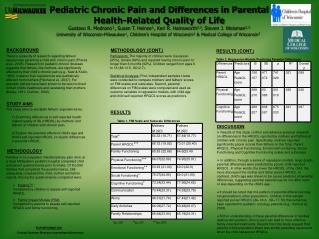
Dyadic Patterns of Parental Perceptions of Health-Related Quality of Life Gustavo R. Medrano & W. Hobart Davies University of Wisconsin-Milwaukee. BACKGROUND. METHODOLOGY (CONT.). RESULTS (CONT.) Table 2. Selected Regression Models Predicting Parental Differences.

E N D
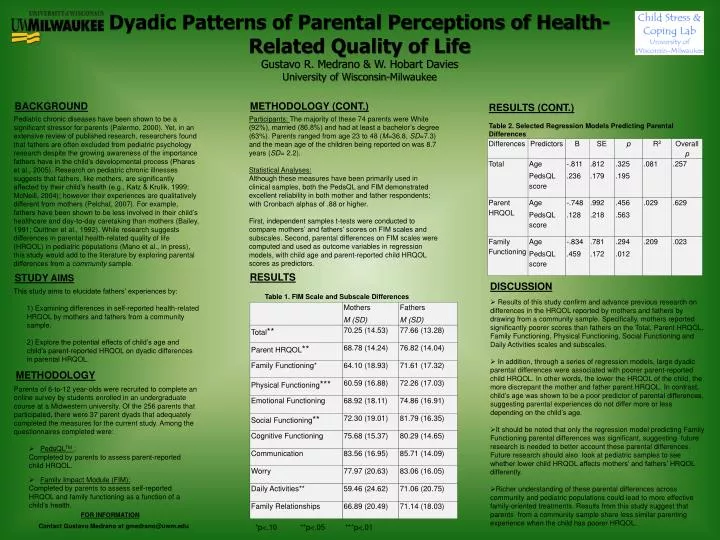
Dyadic Patterns of Parental Perceptions of Health-Related Quality of Life Gustavo R. Medrano & W. Hobart Davies University of Wisconsin-Milwaukee BACKGROUND METHODOLOGY (CONT.) RESULTS (CONT.) Table 2. Selected Regression Models Predicting Parental Differences Pediatric chronic diseases have been shown to be a significant stressor for parents (Palermo, 2000). Yet, in an extensive review of published research, researchers found that fathers are often excluded from pediatric psychology research despite the growing awareness of the importance fathers have in the child’s developmental process (Phares et al., 2005). Research on pediatric chronic illnesses suggests that fathers, like mothers, are significantly affected by their child’s health (e.g., Katz & Krulik, 1999; McNeill, 2004); however their experiences are qualitatively different from mothers (Pelchat, 2007). For example, fathers have been shown to be less involved in their child’s healthcare and day-to-day caretaking than mothers (Bailey, 1991; Quittner et al., 1992). While research suggests differences in parental health-related quality of life (HRQOL) in pediatric populations (Mano et al., in press), this study would add to the literature by exploring parental differences from a community sample. Participants: The majority of these 74 parents were White (92%), married (86.8%) and had at least a bachelor’s degree (63%). Parents ranged from age 23 to 48 (M=36.8, SD=7.3) and the mean age of the children being reported on was 8.7 years (SD= 2.2). Statistical Analyses: Although these measures have been primarily used in clinical samples, both the PedsQL and FIM demonstrated excellent reliability in both mother and father respondents; with Cronbach alphas of .88 or higher. First, independent samples t-tests were conducted to compare mothers’ and fathers’ scores on FIM scales and subscales. Second, parental differences on FIM scales were computed and used as outcome variables in regression models, with child age and parent-reported child HRQOL scores as predictors. RESULTS Table 1. FIM Scale and Subscale Differences STUDY AIMS DISCUSSION This study aims to elucidate fathers’ experiences by: 1) Examining differences in self-reported health-related HRQOL by mothers and fathers from a community sample. 2) Explore the potential effects of child’s age and child’s parent-reported HRQOL on dyadic differences in parental HRQOL. • Results of this study confirm and advance previous research on differences in the HRQOL reported by mothers and fathers by drawing from a community sample. Specifically, mothers reported significantly poorer scores than fathers on the Total, Parent HRQOL, Family Functioning, Physical Functioning, Social Functioning and Daily Activities scales and subscales. • In addition, through a series of regression models, large dyadic parental differences were associated with poorer parent-reported child HRQOL. In other words, the lower the HRQOL of the child, the more discrepant the mother and father parent HRQOL. In contrast, child’s age was shown to be a poor predictor of parental differences, suggesting parental experiences do not differ more or less depending on the child’s age. • It should be noted that only the regression model predicting Family Functioning parental differences was significant, suggesting future research is needed to better account these parental differences. Future research should also look at pediatric samples to see whether lower child HRQOL affects mothers’ and fathers’ HRQOL differently. • Richer understanding of these parental differences across community and pediatric populations could lead to more effective family-oriented treatments. Results from this study suggest that parents from a community sample share less similar parenting experience when the child has poorer HRQOL. METHODOLOGY • Parents of 6-to-12 year-olds were recruited to complete an online survey by students enrolled in an undergraduate course at a Midwestern university. Of the 256 parents that participated, there were 37 parent dyads that adequately completed the measures for the current study. Among the questionnaires completed were: • PedsQLTM: • Completed by parents to assess parent-reported child HRQOL. • Family Impact Module (FIM): • Completed by parents to assess self-reported HRQOL and family functioning as a function of a child’s health. FOR INFORMATION Contact Gustavo Medrano at gmedrano@uwm.edu *p<.10 **p<.05 ***p<.01