Download
1 / 64
660 likes | 911 Views
慢性疾病的運動處方 Exercise Prescription for Chronic Disease. 陳俊忠 Jin Jong Chen MD, PhD 陽明大學運動健康科學研究中心主任 台灣運動健康學會理事長. Questions:. 為什麼要討論慢性病 ? 運動有用嗎 ?. M.D. = M anager of D ’s. D eath 死亡. D isability 失能. D iscomfort 不適. D ollar Cost 費錢.

E N D
慢性疾病的運動處方Exercise Prescription for Chronic Disease 陳俊忠 Jin Jong Chen MD, PhD 陽明大學運動健康科學研究中心主任 台灣運動健康學會理事長
Questions: • 為什麼要討論慢性病? • 運動有用嗎?
M.D. = Manager of D’s Death 死亡 Disability 失能 Discomfort 不適 Dollar Cost 費錢
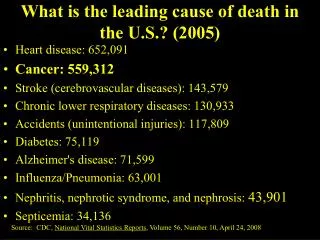
Leading Causes of Death , Taiwan Area, 1992 and 2002 (Bureau of health promotion department of health ,Taiwan ,R.O.C.)
現代文明社會國民致病致死的因素 • 現有健康醫療體系的不健全(10%) • 行為因素與不健康的生活型態(50%) • 環境引起的危害(20%) • 人體的生物因素(20%)
現代社會文明病的特徵 • 初期沒有自覺症狀 • 放置不管病情會日益惡化不會自然痊癒 • 疾病的成因發病的機轉很複雜 • 經常合併其他文明病同時存在 • 和老化現象有關
可防範的危險 • 許多遺傳性疾病,一方面和先天因素有關,一方面則來自後天習慣的影響,例如:心臟病、高血壓、糖尿病、乳癌、結腸癌、酗酒、憂鬱等。 • 家族健康史,甚至全家定期健康檢查,有其意義
身體活動或體適能和慢性疾病相關研究結果摘要身體活動或體適能和慢性疾病相關研究結果摘要 疾病或狀況 研究數量 活動量或組別效益 總死亡率 *** ↓↓↓ 冠狀動脈疾病 *** ↓↓↓ 高血壓 ** ↓↓ 肥胖 *** ↓↓ 中風 ** ↓ 周邊血管疾病 * → 非依賴糖尿病 * ↓↓ 退化性關節炎 * → 骨質疏鬆症 ** ↓↓ 研究數量:*少於五篇 **5-10篇 ***多於10篇 效益:→沒有差別 ↓有某些差別 ↓↓相當有效益 ↓↓↓非常有效益
身體活動或體適能和慢性疾病相關研究結果摘要身體活動或體適能和慢性疾病相關研究結果摘要 疾病或狀況 研究數量 活動量或組別效益 癌症 大腸癌 *** ↓↓ 直腸癌 *** → 胃癌 * → 乳癌 * ↓ 前列腺癌 ** ↓ 肺癌 * ↓ 胰臟癌 * → 研究數量:*少於五篇 **5-10篇 ***多於10篇 效益:→沒有差別 ↓有某些差別 ↓↓相當有效益 ↓↓↓非常有效益
Death Rates and RR for Selected Mortality Predictors, Men, ACLS Death rates and relative risks are adjusted for age and examination year Relative risks are for risk categories shown here compared with those not at risk on that predictor Blair SN et al. JAMA 1996; 276:205-10
Cardiorespiratory Fitness, Risk Factors and All-Cause Mortality, Men, ACLS # of risk factors Risk Factors current smoking SBP >140 mmHg Chol >240 mg/dl Cardiorespiratory Fitness Groups *Adjusted for age, exam year, and other risk factors Blair SN et al. JAMA 1996; 276:205-10
Fitness and CVD Mortality in Blood Pressure Groups, ACLS Men P=0.01 P=0.02 P=0.0003 *Adjusted for age and examination year Church T et al. Am J Cardiol In press 2001
冠狀動脈疾病致死危險因子歸因與社會成推估(美國)冠狀動脈疾病致死危險因子歸因與社會成推估(美國) 危險因子 危險歸因 社會成本推估 (%)(N=593.111) (美金:兆) 身體不活動34.6 $5.7 肥胖32.1 $5.3 抽煙25.0 $4.1 高血壓28.9 $4.7 高血脂42.1 $7.0 (總膽固醇≧200μ g/dl)
冠狀動脈疾病危險因子盛行率危險歸因成本效益(美國)冠狀動脈疾病危險因子盛行率危險歸因成本效益(美國) 危險因子 盛行率(%) 危險歸因(%) 成本效益 缺乏身體活動58.0 34.6 $11,313/QALY 高血壓18.0 28.9 $25,000/QALY 抽煙 25.5 25.0 $21,947/QALY 肥胖23.0 32.1 沒有相關資料 高血脂37.0 42.7 $28,000/QALY (總膽固醇≧200μ g/dl) QALY:沒有疾病的壽命年 $某數/QALY:延長QALY一年採用減少危險因子所需費用 1METs=3.5ml/min/kg 金額/QALY:每增加一年有活動壽命的成本
Questions: • 如何早期篩檢高危險群? • 健康體能有何重要性?
新世紀健康檢查 健康體能及心理健康納入健康檢查內涵 • 確立積極性健康指標 • 偵測慢性病危險因子 • 創造衛生教育契機 • 改善醫療刻板印象 公共衛生研究所規劃培訓人才 署立醫院、衛生所推動執行
Diabetes risk factors checklist • Hypertension, • Obesity, • Hyperglycemia, • Hypertriglyceride, • Age, • DM family history, • Gestational diabetes
OGTT Glucose Tolerance and Insulin Responses According to Type 2 Diabetes Risk Level Plasma Glucose Concentration Plasma Insulin Concentration
Insulin Sensitivity and Insulin Secretion According to Type 2 Diabetes Risk Level † ‡ ‡ ‡ ‡ ‡ δ †§# †§#
Fitness Measurement by a Modified Three-minute Step Test: its Clinical Relevance to Risk of the Metabolic Syndromes Tsai M.W. Liou Y.M.* Wang T.J. Lee H.J. Lin S.P. Chen C.J. Chen J.J. Exercise and Health Science Institute, Institute and Faculty of Physical Therapy, * Institute of Community Nursing, National Yang Ming University, Taipei, Taiwan
Actual number of Steps Duration of Test (seconds) X 100 X ( Sum of Recovery HR ) X 2 24 (steps/min) × Duration of Test (min) Modified three-minutes step test • 35-cm height bench • 96 counts/min in speed • Duration : 3 minutes • Measures: • 30-second recovery HR at 1’,2’,3’ after test • duration of test • number of steps during test • Modified Physical Efficiency Index (mPEI) =
Cutoff Points of the Fitness Category Based on the distribution of modified PEI Least-Fit : below the first quartile (mPEI < 49.3) Moderate-Fit : within interquartile range (mPEI= 49.4 ~ 59.6) Most-Fit : above the third quartile (mPEI > 59.6)
Metabolic Syndromes -- Cutoff Point of Risk Category • Metabolic syndrome is a cluster of related metabolic abnormalities: (based on the criteria of ATP III, 2001) • Hypertension:SBP >= 130 mmHg or DBP >= 85 mmHg • Hyperglycemia:Fasting Plasma Glucose >=110 mg/dL • Dyslipidemia: • Hypertriglycerides:Serum Triglycerides>=150 mg/dL • Low HDL:men < 40 mg/dL, female < 50 mg/dL • Central Obesity :Waist girth men > 100 cm female > 88 cm
Risk Association of the Metabolic Risk Factors and Fitness by gender a SOR= Odds Ratio adjusting by age. The most-fit category was as a reference indicator.
Risk Association of modified Physical Efficiency Index and Numbers of Metabolic Abnormalities * -- Least-Fit vs Most-Fit -- Moderate-Fit vs Most-Fit * * Age-adjusted Odds Ratio * * * Male * * * * Female The number of metabolic abnormalities
Physical fitness measurements Body mass index (BMI) were used to categorize the subjects into: • underweight (UW, BMI<18.5) • normal (N, 18.5 < BMI > 24) • overweight (OW, 24 < BMI > 27) • obese (O, BMI > 27)).
OGTT Glucose Tolerance and Insulin Responses According to BMI Categories Plasma Insulin Concentration Plasma Glucose Concentration
Insulin Sensitivity and Insulin Secretion According to BMI Categories * * ** ** ** **
Insulin Sensitivity and Insulin Secretion According to VO2 Max Categories * *
Insulin Sensitivity and Insulin Secretion According to BMI Categories & Fitness Levels ** ** ** **
Early Detection of Pre-Type 2 Diabetes • Stage 0: normal glucose tolerance and euinsulinemia with increasing insulin resistance MR • Stage 1: normal glucose tolerance due to compensating hyperinsulinemia to overcome the mild insulin resistance. HR • Stage 2: impaired glucose tolerance due to the severe insulin resistance VHR Insulin resistance 0 3 1 Fasting glucose 2 Insulin secretion Type 2 DM Normal Time frame IFG 1.8Y 3.3Y
Questions: • 為什麼會肥胖? • 肥胖怎麼辦?
以人類演化的觀點看肥胖 • 三酸甘油酯與生存 • 糧食中斷為人類生存之主要挑戰 • 三大能源儲存庫 • 肌肉組織、脂肪組織、肝臟 • 勞動與能源分配的關係 • 肌肉組織具有能源儲存的「調整能力」 • 靠勞動生存是百萬年來的人類演化結果
重要性 • 肥胖可直接導致「抗胰島素現象(insulin resistance)」 • 「抗胰島素現象」- pathogenic origin • 第二型糖尿病、高血壓、中風、心臟病、某些型態的癌症 (Revean, 1988; Facchini et al., 2001) • 門診費用每年高達400億以上 • 全球性肥胖人口突增 且持續增加 • 台灣成人平均體重五年內增加2-4公斤
環境因素 • 與飲食熱量及高脂肪飲食未發現顯著關連 (目前無法確定) • Prentice & Jebb. BMJ, 311, 437-439, 1995. • Willett & Leibel. American Journal of Medicine, 113 Suppl 9B, 47S-59S, 2002. • 與身體活動量減少有關 • Kopelman. Nature, 404,635-643, 2000. • Numerous studies………
身體活動量與產業轉型 • 產業大幅轉型、勞力產業人口銳減 • 交通便捷性突增 • 室內活動吸引力的增加 (電視與電腦的發明) • 戶外活動時間減少
肥胖影響身體胰島素敏感度 • 第二型糖尿病與肥胖呈高度相關 • 由於肥胖造成抗胰島素現象 • 機轉目前並不明朗 • 脂肪組織能源儲存狀態,調節全身能源儲存狀態!? • 脂肪組織與肌肉組織存在「對話機制(dialog mechanism)」
抗胰島素現象(Insulin Resistance) • 指身體對胰島素敏感度與反應度下降的現象(Revean, 1988) • 嚴重抗胰島素現象直接導致糖尿病(Revean, 1988) • 第二型糖尿病與老年代謝疾病的共同起源(Revean, 1988; Facchini et al., 2001) • 與肥胖及老化有關 (Rowe etal., 1988) • 規律運動可防止「抗胰島素現象 」(Review in Ivy, 1997)
運動可防止肥胖 • 運動增加肌肉組織血液供應藉以減少脂肪組織能源供應 • 運動降低脂肪細胞三酸甘油酯的儲存能力, 藉由改變LPL活性 • 運動增加肌肉量, 基礎代謝率與肌肉量成正比 • 運動訓練者在休息時脂肪使用比例較高 • 運動訓練者脂肪組織對兒茶酚氨(Catecholamine) 敏感度高, 脂肪易被分解 • 「重量訓練」較「有氧訓練」效果快 • 三餐安排於運動後, 效果較運動後四小時佳
運動員 缺乏運動者
Questions: • 運動有那麼重要嗎? • 慢性病如何運動?
運動對糖尿病的三級預防都有效益 • 5990位賓大校友由1962至1976年長達15年之前瞻性世代研究顯示:每增加2000 kcal/weeks的運動能量消耗可以減少24%第二型糖尿病的危險 Helmrich, Ragland, Paffenbarger,(1994) • 對5771個中國人進行社區實驗,發現運動、飲食或二者均有助於降低葡萄糖耐受不良(IGT)發展為非胰島素依賴型糖尿病(NIDDM),說明了運動對糖尿病高危險群也有預防的效益 Pan (1997) • 以自我配速調整的12周走路運動,得以降低糖尿病患的血糖及血脂,指出運動可以減緩對糖尿病合併症的發生 Walker (1999)
第2型糖尿病患者的運動處方建議 摘自:American College of Sports Medicine. ACSM’s Resource Manual for Guidelines for Exercise Testing and Prescription (3rd ed.). Williams & Wilkins: Baltimore, 1998.
結構式運動介入的限制 • 嚴格的實驗情境可以得到較高的內在效度,但也得付出較低外在推廣效度的代價(Neuman, 1999) • 實驗室中相對讓受測者參與設計流程與處方的機會有限,不允許太多的更動 • 社區衛教與共同照護,卻必須確保民眾的充分參與及鼓勵民眾自決(empower)
糖尿病患進行運動防治的實務困難 • 先前的運動意願不高、活動量不足 • 有80%比理想體重多20%達到肥胖的程度 • 肥胖後運動更困難 • 得病後的合併症影響身體活動能力
完善的糖尿病運動計畫重點 • 個人化 尊重個人選擇、特質:運動喜好、運動型態、現有資源 評估改變的初始動機;對運動、理想體重、肥胖的態度 依改變階段提供合適建議 • 可行性 中等強度可融入生活型態的運動:如走路、騎腳踏車 有回饋、監督系統:如契約;保證金;日記; 密切的電話、信函、網路接觸;每個月回診 建立社會支持系統:病友團體、家族諮詢 • 有效性 中等強度150min/weeks 自我管理、行為修正法 多目標:合併處理肥胖及飲食