Download
1 / 163
1.7k likes | 2.07k Views
High Density Lipoprotein Complexities. Thomas Dayspring, MD, FACP, FNLA Clinical Assistant Professor of Medicine University of Medicine and Dentistry of New Jersey, New Jersey Medical School Diplomate of the American Board of Clinical Lipidology

E N D
High Density Lipoprotein Complexities Thomas Dayspring, MD, FACP, FNLA Clinical Assistant Professor of Medicine University of Medicine and Dentistry of New Jersey, New Jersey Medical School Diplomate of the American Board of Clinical Lipidology Fellow: National Lipid Association North American Menopause Society Certified Menopause Practitioner North Jersey Institute of Menopausal Lipidology Wayne, New Jersey
22 24 26 21 25 20 23 18 CH3 27 12 17 13 16 11 19 CH3 14 15 1 9 2 10 8 5 7 3 OH 4 6 A sterol with 27 carbon molecules with an -OH group at the # 3 position Hydrocarbon tail C27H45OH 4 Hydrocarbon Rings
Foam Cells IDL LDL HDL VLDL Sterols along with triglycerides and phospholipids are trafficked within apoprotein enwrapped particles called lipoproteins It is the apoB particles, > 90% of which are LDLs (LDL-P) that drive atherosclerosis Apolipoprotein B particles Apolipoprotein A-I particles Macrophage
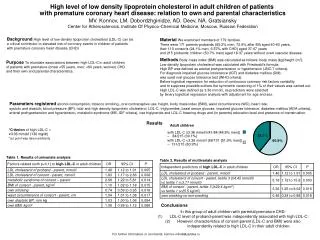
Apoprotein-related MOrtality RISk AMORIS Study • 175,553 patients from screening programs • 98,722 men and 76,831 women • Examined relationship of apoproteins and lipids and prediction of fatal MI • Mean Follow up 66-68 months Wallidius G et al Lancet 2001;358:2026-2033
Apoprotein-related MOrtality RISk AMORIS Study • In multivariate analyses adjusted for age, TC and TG • Apolipoprotein B was a stronger predictor of risk than LDL-C in both sexes ApoB is obviously a marker of atherogenic lipoprotein particles Wallidius G et al Lancet 2001;358:2026-2033
Lab Analysis of ApoB Lipoproteins ApoB Concentration VLDL-P IDL-P LDL-P Chylomicrons VLDLs IDLs LDLs LDL-C TC – HDL-C + VLDL-C VLDL-C TG/5 Non HDL-C TC – HDL-C or VLDL-C + LDL-C ApoB Lipoproteins
Controversy: Is lowering low-density lipoprotein an effective strategy to reduce cardiac risk? Healthcare workers need to consider the possibility that the cholesterol-lowering program has in large part failed to stem the epidemic of CHD and that the well-meaning focus on LDL-C reduction has deflected interest in other therapeutic aspects of lipoprotein treatment that provide equal or greater benefit. This myopic focus on LDL alone is not surprising because, so far, guidelines have not adequately addressed other evidence. Superko HR, & King S. Circulation. 2008;117:560-568
Can High Density Lipoproteins prevent or ameliorate atherosclerosis and if so is that protection dependent on how much cholesterol is within the HDL particle (HDL-C) ?
High Density Lipoproteins Classification
High Density Lipoprotein (HDL) Apo A-I is a surrogate of HDL particle concentration Apo E Apo A Family (A-I, A-II, A-IV, A-V) Triglycerides Apo C (C-I,C-II,C-III) HDLs also serve as a transport vehicle for CETP, LCAT and PLTP Cholesterol ester HDL-C Phospholipids Apo J (clusterin) and D, F and L are also associated with HDL Apo B / Apo A is an advanced TC / HDL-C or LDL-C / HDL-C ratio
High Density Lipoprotein Classification • The HDL is heterogeneous in terms of shape, size, density, composition and surface charge and can be classified: • By density (ultracentrifugation) • By gradient gel electrophoresis (GGE) • By NMR-spectroscopy spectral signals • By surface charge (agarose gel electrophoresis) • By apolipoprotein composition • By dynamic metabolism: isotachoelectrophoresis Barter, Philip et al. Atherosclerosis 2003;168:195-211
HDL1 HDL3 HDL2 HDL5 HDL4 10-13 nm 8.8-10 nm 8.2-8.8 nm 7.8-8.2 nm 7.3-7.7 nm HDL3c HDL2b HDL3b HDL2a HDL3a 10.6 nm 9.2 nm 8.4 nm 8.0 nm 7.6 nm HDL Subpopulations by GGE & NMR NMR Subpopulation Nomenclature Gel Electrophoresis Subpopulation Nomenclature Barter, Philip et al. Atherosclerosis 2003;168:195-211
LDL Sizing by Gradient Gel Electrophoresis HDL-S3GGE™ 2 4 5 1 3 3c 3b 2a 3a 2b Reverse Cholesterol Transport Segmented HDL Subclass Determination
HDL1 HDL3 HDL2 HDL5 HDL4 HDL3c HDL2b HDL3b HDL2a HDL3a Unlipidated apoA-I or phospholipidated prebeta-1 & 2 HDL HDL-cholesterol Concentration Alpha HDLs Alpha 1 Alpha 3 Alpha 4 apoA-II apoA-II apoA-I Alpha 2 apoA-I apoA-II apoA-I apoA-I apoA-I HDL-P reflects the number of α-HDL particles HDL-C primarily reflects cholesterol levels within large, cholesterol-rich particles and lacks sensitivity to detect small cholesterol-poor particles
HDL by Apolipoprotein A Lipoprotein A-I/A-II (LpA-I/A-II) Lipoprotein A-I (LpA-I) Lipoprotein A-II (LpA-II) Apo A-II Apo A-I Most of the LpA-I/A-II are found in the small HDL3 density range, while LpA-I are prominent components of both HDL2 and HDL3 Barter, Philip et al. Atherosclerosis 2003;168:195-211
HDL Subpopulations by Surface Charge • In the first dimension(mobility), there are three ApoA-I HDL subpopulations separated by charge on agarose gel (on the basis of electrophoretic mobilities relative to albumin) • Alpha: α (Rf = 1) mobility similar to albumin • Pre-alpha: Pre-α (Rf > 1) mobility faster than albumin • Pre-beta: Pre-β (Rf < 1) mobility slower than albumin • In the second dimension(size characterization), the particles (12) were differentiated on nondenaturing gel electrophoresis by modal diameters Asztalos BF Biochim Biophys Acta 1992;1169:291-300
HDL Subpopulations by Two Dimension al Electrophoresis and Surface Charge First Dimension Prebeta & alpha (α) migrating apoA-I on agarose gel electrophoresis Second Dimension Separation by size: Nondenaturing concave polyacrylamide gel electrophoresis & immunolocalization albumin Asztalos BF Biochim Biophys Acta 1992;1169:291-300
First Dimension (median Rf) Second Dimension modal diameter (nm) α1 α2 α3 pre-α1 pre-α2 pre-α3 pre-α4 pre-β1a pre-β1b pre-β2a pre-β2b pre-β2c 0.99±.030.93±.041.01±.031.39±.03 1.39±.03 1.39±.031.39±.030.38±.04 0.42±.09 0.76±.02 0.72±.02 0.64±.02 10.97±.109.20±0.187.62±0.2511.05±0.31 9.42±0.21 8.40±0.277.67±.0.155.79±0.18 5.38±0.21 13.74±0.27 12.85±0.14 12.17±0.20 18.2% 29.0% 20.2% 6.5% 7.8% 3.2% 2.5% 3.5% 3.1% 1.8% 2.2% 1.6% HDL Subpopulations by Two Dimensional Electrophoresis and Surface Charge 12 ApoA-I HDL Subpopulations Pre-β 2 alpha a b Pre-α c 1 2 3 4 albumin a b Pre-β 1 % Distribution Asztalos BF Biochim Biophys Acta 1992;1169:291-300
Capillary Isotachophoresis • HDL were separated into three subfractions: • The fast migrating HDL correlated positively with serum apoA-I (P, 0.05) and negatively with triglyceride (P, 0.01) concentrations, • The intermediate migrating HDL involved in HDL-cholesterol delivery and inversely related to LDL particles concentration (P, 0.001), • The slow migrating preb1-HDL. Schlenck A et al. J. Lipid Res. 1999;40:2125–2133
Capillary Isotachophoresis Representative cITP profile of the lipoprotein subfractions separated from a normolipidemic serum. 395 1. fHDL 295 8. sLDL Relative Fluorescence Units (RFU) 195 7. fLDL 6. IDL 2,3. iHDL 5. VLDL 4. sHDL 95 5 5.1 6.1 5.6 Migration Time (min) Schlenck A et al. J. Lipid Res. 1999;40:2125–2133
High Density Lipoproteins What’s New ?
High Density Lipoproteins Despite the preponderance of evidence linking low HDL-C levels to cardiovascular morbidity and mortality, there is no definitive evidence proving that increasing HDL-C levels reduces the incidence of major cardiovascular events. Indeed, major clinical guidelines have avoided providing an HDL-C target, despite some consensus statements that increasing HDL-C levels has merit. Inder M. Singh, Mehdi H. Shishehbor, Benjamin J. Ansell, M AMA. 2007;298(7):786-798
National Cholesterol Education ProgramAdult Treatment Panel III NCEP-ATP III Addendum Low HDL-Cholesterol Although the potential benefit of HDL-raising therapy has evoked considerable interest, currentdocumentation of risk reduction through controlled clinical trials is not sufficientto warrant setting a specific goal value for raising HDL-C. Recent lipid-lowering drug trials provide no new evidence in this regard. Circulation 2004;110:227-239
ApoA-I Containing Lipoproteins Alpha HDLs Mature Immature apoA-I apoA-II apoA-II apoA-I apoA-I apoA-II apoA-I apoA-I HDL3b or H2 HDL3c or H1 HDL3a or H3 HDL2a or H4 HDL2b or H5 α-HDL2 α-HDL3 α-HDL1 α-HDL4 Prebeta HDLs Lp A-I are apoA-I containing HDLs: Lp A-I,A-II are apoA-I and apoA-II containing HDLs There can be from two to four molecules of apoA-I per HDL particle, thus apoA-I is only an approximation of the number (concentration) of HDL particles. ApoA-II is also present , predominantly on the smaller species Unlipidated apoA-I or phospholipidated prebeta-1 & 2 HDL
The Yin and Yang of High Density Lipoprotein Cholesterol The epidemiologic association (of low HDL-C and CVD risk) was thought to work in reverse: raising HDL should prevent coronary artery disease. This simple paradigm remains unproven to date. Jacques GenestJACC. 2008;51;643-644
Association Between Change in HDL-C and CVD Mortality: Meta-regression Analysis • Meta-regression analysis of 108 randomized trials involving 299,310 patients at risk for CVD. • All analyses adjusted for LDL-C showed no association between treatment- induced change in HDL-C and risk ratios for CHD deaths, CHD events, or total deaths. • With all trials included, change in HDL-C explained almost no variability (< 1%) in any of the outcomes Briel, M et al. BMJ 2009;338
Association Between Change in HDL-C and CVD Mortality: Meta-regression Analysis Available data suggest that simply increasing the amount of circulating HDL-C does not reduce the risk of CHD events, CHD deaths, or total deaths. The results support reduction in LDL-C as the primary goal for lipid modifying interventions Briel, M et al. BMJ 2009;338
Association Between Change in HDL-C and CVD Mortality: Meta-regression Analysis Raising HDL-C without considering effects on HDL function seem to have little promise for the prevention of CVD events Future research should prospectively consider the results of assays to measure HDL function and then provide definitive evidence of pharmacological effects of patient important outcomes in long term randomized trials Briel, M et al. BMJ 2009;338
Controversy: Is lowering low-density lipoprotein an effective strategy to reduce cardiac risk? Whether raising HDL by pharmacological intervention that directly targets HDL will reduce cardiovascular risk remains to be proven. It is possible that a low HDL is primarily a marker of risk caused by other factors (eg, metabolic syndrome) and that direct HDL raising will not substantially modify risk. Grundy, Scott. Circulation. 2008;117:560-568
Controversy: Is lowering low-density lipoprotein an effective strategy to reduce cardiac risk? To resolve this question, two things are needed: development of a drug that will effectively raise HDL (without a confounding lowering of apolipoprotein B–containing lipoproteins) and demonstration of the efficacy of such a drug in a morbidity/mortality outcome trial. Until these have been accomplished, the benefit of raising HDL per se remains in the arena of speculation. Grundy, Scott. Circulation. 2008;117:560-568
A New Age of Discovery for Plasma Lipoproteins Somehow, the unstoppable progression of the LDL concept dragged along the notion that its perceived counterpart and nemesis, HDL, would carry equally large opportunities for therapeutic maneuvers in atherosclerosis. Indeed, armed solely with the power of epidemiological observations, the idea that raising one’s plasma HDL cholesterol levels will reduce the risk of a heart attack has become so entrenched in clinical thinking that many doctors switch to target an unproven HDL goal before ‘finishing off’ the LDL villain. Therefore, a current was created for an expectation that any rise in plasma HDL cholesterol would always indicate improved reverse cholesterol transport and enhanced vascular protection. Here, too, we got our share of shocking surprises in the last few months. Sergio Fazio and MacRae Linton Current Opinion in Lipidology 2007, 18:387–388
A New Age of Discovery for Plasma Lipoproteins The most devastating blow, however, was taken by all of us lipidologista, who are now forced to rethink reverse cholesterol transport as a therapeutic target and cannot expect any longer for HDL to follow LDL’s easy street. This means that any target leading to HDL increases must be tested for cardiovascular benefits, and, most importantly, that there may be interventions on HDL that may be beneficial without raising HDL cholesterol or even by decreasing it. Sergio Fazio and MacRae Linton Current Opinion in Lipidology 2007, 18:387–388
Estrogen and HDL All that Glitters Is not Gold “Just because a biomarker is associated with coronary heart disease (CHD) events in epidemiologic studies is not a guarantee that pharmacologically altering the biomarker will result in changes in CHD risk in the anticipated direction. To successfully forecast clinical consequences requires an extremely detailed understanding of the physiology of the biomarker and its regulation. David M. Herrington, and John S. Parks ArteriosclerThrombVasc Biol. 2004;24:1741-1742.
High Density Lipoproteins What is their role in atherogenesis and atheroprotection?
Apoprotein-related MOrtality RISk AMORIS Study • In multivariate analyses adjusted for age, TC and TG • Apolipoprotein B was a stronger predictor of risk than LDL-C in both sexes • Apolipoprotein A-I was protective Wallidius G et al Lancet 2001;358:2026-2033
100 100 80 80 60 60 40 40 20 20 0 0 1.0 1.0 2.0 2.0 1.4 1.4 1.6 1.6 2.2 2.2 2.4 2.4 1.2 1.2 1.8 1.8 National Health And Nutrition Examination Survey III (NHANES) Apolipoprotein A-I Distributions Males Females Mean Level W 146 B 151 White White Cumulative % Cumulative % Black Black Mexican-American Mean Level W 134 B 145 ApoA-I concentration (gm/L) ApoA-I concentration (gm/L) The mean apo A-I concentration in all males was; 7% lower than in females Bachorik BS, et al. Clinical Chemistry 1997;43:12:2364–2378
Atomic models of monomeric lipid-free apoA-I Apolipoprotein A-I • ApoA-I is an exchangeable helical, apoprotein that is the major constituent of HDL • In lipid-free and lipid-bound states, apolipoproteins span multiple conformations, some of which are required for apolipoprotein functions such as: • Binding to lipid surfaces • Interactions with cellular receptors, lipid transporters, charged ligands • Enzyme activation Olga Gursky. Curr Opin Lipidol 2005;16:287–294. Davidson WF & Silva G. Curr Opin Lipidol 2005;16;295-300.
Apoprotein-related MOrtality RISk AMORIS Study • In multivariate analyses adjusted for age, TC and TG • Apolipoprotein B was a stronger predictor of risk than LDL-C in both sexes • Apolipoprotein A-I was protective • The values for Apo B and the ApoB/ApoA-I ratio were strongly and positively related to risk of fatal MI in men and women Wallidius G et al Lancet 2001;358:2026-2033
Potentially Modifiable Risk Factors Associated with Myocardial Infarction The INTERHEART Study Odds of myocardial infarction according to ApoB/ApoA1 ratio. 8 A standardized case-control study of acute myocardial infarction in 52 countries, representing every inhabited continent. 4 Odds Ratio (99% CI) 2 1 0.75 2 10 3 9 8 1 4 7 6 5 ApoB/A-I ratio (deciles) Number of controls 1210 1206 1208 1207 1210 1209 1207 1208 1208 1209 Number of cases 435 496 610 720 790 893 1063 1196 1366 1757 Median 0.43 0.53 0.60 0.66 0.72 0.78 0.85 0.93 1.04 1.28 15 ,152 cases and 14, 820 controls were enrolled. Yusef S et al. Lancet 2004;364:937-952
1.68 - 4.21 1.47 - 3.25 5.54 – 18.1 4.34 – 19.3 4.22 – 5.53 3.25 – 4.33 Men Women Framingham Offspring Heart Study 35 Tertiles of TC/HDL-C 30 Women 25 Men 20 15 20 Year Incidence (%) 10 5 0 High Cholesterol Low Cholesterol T-3 T-2 T-2 T-1 T-3 T-1 B Nam, WB. Kannel, and RB. D’Agostino, (Am J Cardiol 2006;97:372–375)
Lipids, Lipoproteins & Apolipoproteins as Markers of risk of MI in 52 Countries in The INTERHEART Study 8.00 ApoB/ApoA-I TC/HDL-C Risk of MI for increasing decile medians (adjusted for age, sex and region) of ratios of apoB/ApoA-I and TC/HDL-C 4.00 ApoB/ApoA-I Odds ratio (95% CI) 2.00 TC/HDL-C 1.00 1 2 -1 0 Decile Median (SD distance from overall median) 8 1 6 9 2 7 10 4 3 5 ApoB/ApoA-I 0.43 0.53 0.60 0.66 0.72 0.78 0.85 0.93 1.04 1.28 TC/HDL-C 2.74 3.37 3.82 4.23 4.64 5.08 5.58 6.21 7.15 9.20 McQueen M et al. Lancet 2008;372:224-233
High Density Cholesterol: The Editor’s Roundtable TC/HDL-C Ratio Dan Rader • I am not a fan of lipid ratios. If the HDL-C is high, should there be no worry about a high LDL-C? • The ratio is based on large population studies, using few people with high HDL-C levels • It is therefore uncertain whether ratios even apply to individuals with high HDL-C Scott Grundy • Using ratios depends on the validity of the theory that HDL neutralizes LDL, which is not supported by the evidence. LDL is an atherogenic lipoprotein, and the higher it is the more likely atherosclerosis is present. To expect HDL to block the atherosclerotic effects of LDL may be wishful thinking • Although HDL might play some role in mitigating the effects of LDL, HDL may not be truly protective against high LDL. Vincent Friedewald, H Bryan Brewer, Scott Grundy, Daniel Rader and William Roberts. Amer J Cardiol 2007;99:1698-1705
Lipid Concentrations HDL cholesterol (HDL-C) is the cholesterol trafficked within all of the high density lipoproteins in a deciliter of plasma HDL-C is determined analytically and does not require fasting
High Density Lipoprotein Cholesterol: The Editor’s Roundtable Dan Rader • Plasma HDL-C is the least accurate of standard lipid measurements • Performed correctly, which is true with large labs, HDL-C accuracy is ± 10% • You do not make a treatment recommendation based on a single measurement of HDL-C. A low HDL-C or one that falls unexpectedly should be confirmed with at least one repeat measurement • Dr William Roberts: • An accuracy or ± 10% could give errors of up to 4 mg/dL Vincent Friedewald, H Bryan Brewer, Scott Grundy, Daniel Rader and William Roberts. Amer J Cardiol 2007;99:1698-1705
HDL-cholesterol Concentration HDL-C reflects the cholesterol being trafficked within all of the HDL particles per deciliter of plasma Alpha HDLs apoA-I apoA-II apoA-II Mature Immature apoA-I α-1 α-3 apoA-I apoA-II apoA-I apoA-I α4 α-2 Prebeta HDLs HDL-C primarily reflects cholesterol levels within large, cholesterol-rich particles and lacks sensitivity to detect small cholesterol-poor particles Unlipidated apoA-I or phospholipidated prebeta-1 & 2 HDL Kontush A & Chapman J. Pharm Rev. 2006;58:342-374
Framingham Offspring Study (n = 3,467) Relations of HDL Subclasses and HDL-P to HDL-C For HDL-C < 40 mg/dL, increasing HDL-C is accounted for by increases in levels of all three HDL subclasses, but primarily small HDL. Increases in HDL-C beyond 40 mg/dL are due primarily to changes in HDL particle composition, with large HDL increasing steadily at the expense of decreasing numbers of the smaller HDL subclasses. This is probably due to a product-precursor relationship between these species. Total HDL-P 35 30 25 Small HDL-P 20 HDL Particle Number (HDL-P) in umol/L 15 10 Medium HDL-P 5 Large HDL-P 0 20 30 40 50 60 70 80 90 100 HDL Cholesterol mg/dL Lowess plot: smoothed levels Cromwell, WC. Otvos JD. In Davidson MH, Toth PP, Maki K. eds Therapeutic Lipidology. Totowa, NJ, Human Press
Multiethnic Trial of Atherosclerosis Quantiles of Total HDL-P Total HDL-P is the sum of the small, medium and large HDL particle concentrations Not counted are unlipidated apoA-I and pre-beta HDL particles, which typically make up 5% of HDL particles
High Density Lipoproteins Reduced HDL-C
Men Women National Health And Nutrition Examination Survey III (NHANES): Distribution of Low HDL-C Bottom Tertile of Population 16 • < 40/50 mg/dL men/women are the bottom tertile of population 14 12 10 8 % of the Population • <20 mg/dL occurs in 1/200 men & 1/400 women 6 4 2 • <10 mg/dL occurs in ~ 1/20,000 0 5-9 30-34 10-14 15-19 35-39 20-24 25-29 HDL-C (mg/dL) Miller M & Zahn M. Curr Opin Cardiol 2004;19:380-384
National Cholesterol Education ProgramAdult Treatment Panel III NCEP-ATP III Risk of Low HDL-C Evidence statement A low HDL cholesterol level is strongly and inversely associated with risk for CHD NCEP JAMA 2001;285:2486 Final Report Circulation 2002;106:3143-3421