Download
1 / 1
10 likes | 260 Views
Do offending and non-offending adolescents’ share the same vulnerability factors for self-harm? Evidence from a nurse-led self harm service. Tony Kelly 1 , Robert Young 2 & Eileen McCafferty 1 1 Adolescent Self harm Service, GG&C NHS, Glasgow, G5 0RE, UK

E N D
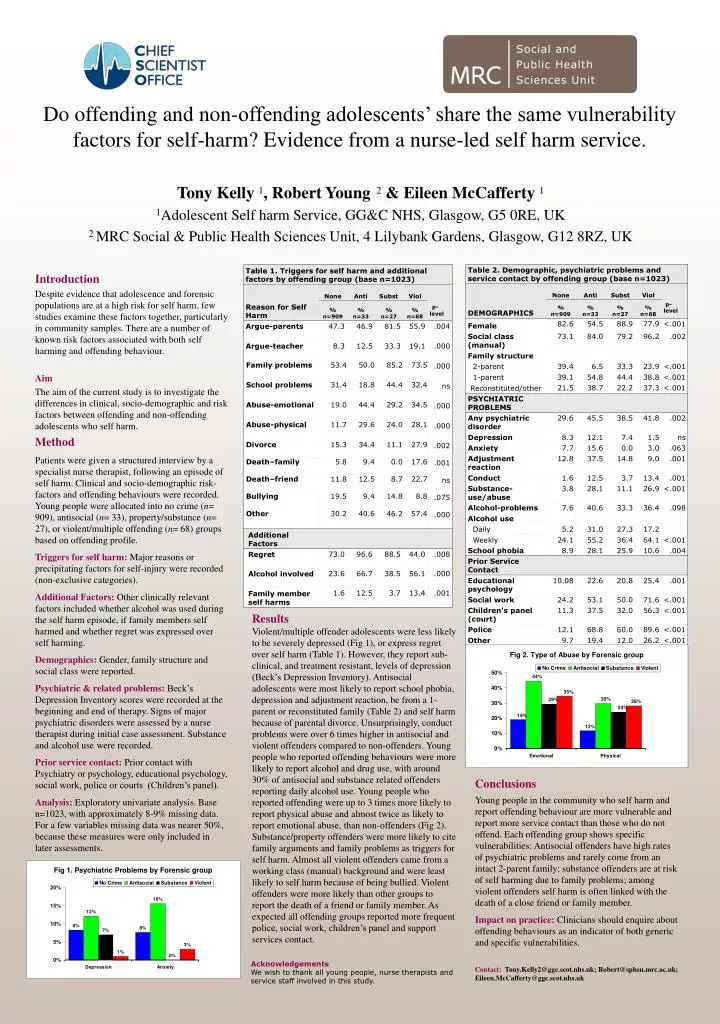
Do offending and non-offending adolescents’ share the same vulnerability factors for self-harm? Evidence from a nurse-led self harm service. Tony Kelly 1, Robert Young2 & Eileen McCafferty 1 1Adolescent Self harm Service, GG&C NHS, Glasgow, G5 0RE, UK 2 MRC Social & Public Health Sciences Unit, 4 Lilybank Gardens, Glasgow, G12 8RZ, UK Introduction Despite evidence that adolescence and forensic populations are at a high risk for self harm, few studies examine these factors together, particularly in community samples. There are a number of known risk factors associated with both self harming and offending behaviour. Aim The aim of the current study is to investigate the differences in clinical, socio-demographic and risk factors between offending and non-offending adolescents who self harm. Method Patients were given a structured interview by a specialist nurse therapist, following an episode of self harm. Clinical and socio-demographic risk-factors and offending behaviours were recorded. Young people were allocated into no crime (n= 909), antisocial (n= 33), property/substance (n= 27), or violent/multiple offending (n= 68) groups based on offending profile. Triggers for self harm: Major reasons or precipitating factors for self-injury were recorded (non-exclusive categories). Additional Factors: Other clinically relevant factors included whether alcohol was used during the self harm episode, if family members self harmed and whether regret was expressed over self harming. Demographics: Gender, family structure and social class were reported. Psychiatric & related problems: Beck’s Depression Inventory scores were recorded at the beginning and end of therapy. Signs of major psychiatric disorders were assessed by a nurse therapist during initial case assessment. Substance and alcohol use were recorded. Prior service contact: Prior contact with Psychiatry or psychology, educational psychology, social work, police or courts (Children’s panel). Analysis: Exploratory univariate analysis. Base n=1023, with approximately 8-9% missing data. For a few variables missing data was nearer 50%, because these measures were only included in later assessments. Results Violent/multiple offender adolescents were less likely to be severely depressed (Fig 1), or express regret over self harm (Table 1). However, they report sub-clinical, and treatment resistant, levels of depression (Beck’s Depression Inventory). Antisocial adolescents were most likely to report school phobia, depression and adjustment reaction, be from a 1-parent or reconstituted family (Table 2) and self harm because of parental divorce. Unsurprisingly, conduct problems were over 6 times higher in antisocial and violent offenders compared to non-offenders. Young people who reported offending behaviours were more likely to report alcohol and drug use, with around 30% of antisocial and substance related offenders reporting daily alcohol use. Young people who reported offending were up to 3 times more likely to report physical abuse and almost twice as likely to report emotional abuse, than non-offenders (Fig 2). Substance/property offenders were more likely to cite family arguments and family problems as triggers for self harm. Almost all violent offenders came from a working class (manual) background and were least likely to self harm because of being bullied. Violent offenders were more likely than other groups to report the death of a friend or family member. As expected all offending groups reported more frequent police, social work, children’s panel and support services contact. Conclusions Young people in the community who self harm and report offending behaviour are more vulnerable and report more service contact than those who do not offend. Each offending group shows specific vulnerabilities: Antisocial offenders have high rates of psychiatric problems and rarely come from an intact 2-parent family; substance offenders are at risk of self harming due to family problems; among violent offenders self harm is often linked with the death of a close friend or family member. Impact on practice: Clinicians should enquire about offending behaviours as an indicator of both generic and specific vulnerabilities. Contact: Tony.Kelly2@ggc.scot.nhs.uk; Robert@sphsu.mrc.ac.uk; Eileen.McCafferty@ggc.scot.nhs.uk Acknowledgements We wish to thank all young people, nurse therapists and service staff involved in this study.