Download

1 / 29
290 likes | 375 Views
WP 5 – Case Material Barrie Dowdeswell Director of Research, ECHAA. Case material - Purpose. Review the effectiveness of the SF process through examination of a cross section of case studies (ESF / ERDF) Programme cycles, 2000/6, 2007/13 Thematic focus Geographical spread

E N D
WP 5 – Case Material Barrie Dowdeswell Director of Research, ECHAA
Case material - Purpose • Review the effectiveness of the SF process through examination of a cross section of case studies (ESF / ERDF) • Programme cycles, 2000/6, 2007/13 • Thematic focus • Geographical spread • Context, Social Cohesion - Health Inequalities, Health is Wealth, Modernisation • Aim, provide evidence to support improvement in the process and to provide knowledge and competency development support to relevant member states and regions • Methodology: • On site interviews and evaluation – transcript based • Desktop research • Thematic analysis and Integration with the EuregioIII scientific paper • Evidence for EIII workshops and masterclasses • Web based resource and ongoing reference ‘library’ • Reports and publications
Case studies Asset based Modernisation eHealth / ICT Quality and Efficiency Brandenburg, Germany, changing focus and locus,the patient as co-producer of care Sicily, needs assessment Finland, Lapland, remote population telecare service delivery & the patient as co-producer of care Slovenia, whole systems ICT investment • Greece, Cancer Centre • Malta, Cancer Centre • Portugal (Saude) Masterplan, (plus) • Hungary Masterplan (plus) • Estonia, Hospital Reconfiguration • Sicily, Technology Diffusion • Greece, Mental Health Services Non SF comparators have been identified (already available on the web site) to provide benchmarks for evaluation, wider range at: Capital investment for health: case studies from Europe. World Health Organization, on behalf of the European Observatory on Health Systems; 2009.http://www.euro.who.int/en/home/projects/observatory/publications/studies/capital-investment-for-health.-case-studies-from-europe
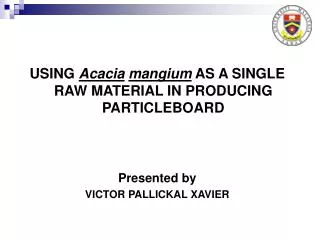
Health and the State / Region‘Health is wealth’ or ‘Health as Cost’ genetics lifestyle labour supply education productivity HEALTH healthcare education capital formation wealth environment other socio- economic factors ECONOMIC OUTCOMES McKee et al LSHTM
An accelerating and increasingly complex trajectory of change in healthcare in the EU The patient as co-producer of care High Intersectoral investment Public Private Partnerships Transformational change Complexity & risk Technology diffusion Modernisation Quality improvement Cumulative growth Incremental change Low Health transitions Credit crisis Deficit reduction Age gap pensions crisis 2000/6 2007/13 20/20 All happening within the current cycle
Europe 2020 – health is not a specific, but more an implicit feature of the strategy document; but ---
Overall ranking of EU Health systemsAn issue of social cohesion The ‘12’
Serious affordability problems for healthcare – in particular the 12 Growth CEE Per-capita spending, EU A potential risk to fiscal governance
Health Inequalities, avoidable mortality, questions and sensitivities – Subsidiarity Variations in (cervical) cancer survival rates 1998 - 2008 Source: OECD health data 2010
Lisbon Strategy evaluation document • “Earmarking of Structural Funds has helped mobilise considerable investments for growth and jobs although there is further to go” • Need to enhance policy effectiveness • Difficulties with the process • Weak capacity • Lack of strategic approach • Poor integration of process • Weak outcome assessment • Need to strengthen leverage – “through financial engineering” Euregiofindings reflect the Lisbon evaluation and add further specific insight
Case studies - examples • Brandenburg Germany – eHealth • The patient as co-producer of care / change • Sicily, Italy - Clinical Technology Investment • Evidence based investment / masterplanning • Greece – Mental Health • Transformational service delivery / change
Brandenburg / GermanyChanging the axis of regional healthcare The patient as co-producer of care Reshaping health services (following reunification) Support from structural funds, 2000-2006 regional development convergence region: Reduce health inequality Wider economic development New medical technology innovation The Region – core problems High unemployment rate, poor access to higher education Run-down rural infrastructure; need for modernisation (generic) Previous (biased) healthcare investment strategies: Closure of previously state run polyclinics in favour of single physicans offices Preferred investment into ‘big hospitals‘ Neglecting accessibility and dissemination
Existing healthcare challenges Legacy offormerhealthcaresystem Localagendas Underinvestment & lack ofresources “Brandenburg (sharingstructuralsimilaritieswiththenewmemberstates) in someaspectsis a laboratoryforhealthinvestmentsasmeansforstimulatingnew regional policy.“ Lack of trained workforce Funding of large scale hospitals “I think the true philosophy behind this is, if you have limited amount of money, say in funds or whatever, you can go and look and say, okay, the big towns, the big cities will get the most. The philosophy, in contrary should be to say, medicine has to go to the people where they live. It is in the 21st century not true that MRI or heart surgery is so spectacular that it only could be in great metropolitan areas.” Lack of appropriate health infrastructure in rural areas Need to introduce innovation and telemedicine
Project aims and emerging outcomes Move more care into locally and more accessible community settings – the patient in greater control Increase accessibility of health equipment, technology diffusion Move towards new technology/introduction of telemedicine, innovation Competency development, professionals and citizens “What to do”: “Whole system change (away from big hospitals into community settings; shift towards prevention and rehabilitation Putting the patient back in charge – an issue of belief and trust Increase awareness of interactions between different system components, and stakeholder groups” – how does it all fit together?
Sicily, Italy: current healthcare system problems • Overspending • Administration inefficiency (need for accountability) “It is very well built, but managed in a terrible way.” • High pharmaceutical consumption (a typical) new (medicines) technology diffusion problem • Ageing population • High passive mobility (patients get treated in other regions of Italy) • Out-dated, insufficient clinical technology • Lack of resources • Inequality (limited access to care, especially pronounced in rural • regions)
Sicily: Multiple project objectives • Introducing Centralized Tenders – procurement efficiency • Cost containment • Trimestral Performance Monitoring and Evaluation • Fill gaps in care (& tackle inequality) – health access in rural areas • Upgrade emergency services • Laboratories: centralise diagnostic capacity and improve quality Reshaping hospital network, territorial and social care • Organizational innovation (hub and spoke networks - hospital-territory) • Technological innovation • Improve infrastructural facilities • Integrate services, residential, public-private joint venture
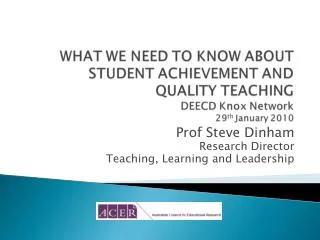
Project plan – before and after Radiotherapy 2009 Radiotherapy 2012
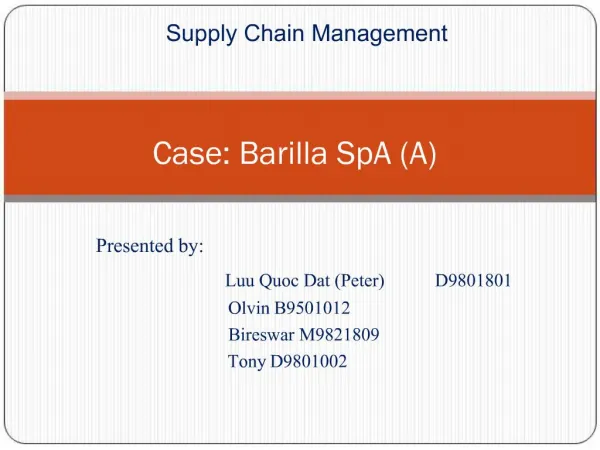
An EU comparative viewCapital investment (MRI) it is not how many - but effectiveness of return on investment Waiting times 30 1 9 months One week 4 months Scanner range 1 to 30 per million population European recommendation 10 to 12 per million
Sicily: identified SF project issues (1) Lack of strategic alignment “There is a need to integrate the master plan in investments at regional and local level.” Missing outcome measures Inappropriate quality measures Poor integration of processes Product hospitals and facilities based on outmoded principles “[...] avoid funding and building (just) prestigious projects.“
Identified SF process challenges (2) • Time consuming • Very prescriptive • Missing guidance from EU and government • Administrative procedures a barrier to innovation “ [...] there should be a contest of ideas, choose the projects according to quality [...]“ • Missing alignment of different EU funding streams “[...] seek to reach synergy between ERDF and ESF.““The integration of the different funds, different European funds, should be improved, because now it seems that the division into the assistance of different funds, like the health, and so on, are too sectorial and too limited to itself, and not sufficient integration among them.” • Competing interests in other fields e.g. education
Greece Mental Health Service TransformationPSYCHARGOS B programme Problem • Institutionalised (asylum) care for almost all psychopathologies – large, overcrowded psychiatric hospitals with quality, accessibility, workforce and ‘outmoded’ service issues Target • Replacing institutional care with primary, extramural (local community) and acute care service delivery • Reform stimulated by Greece entry to the EU • Redesign supported by advice from the WHO and EU, but very slow progress in the period 1989 -1998
PSYCHARGOS B programme PSYCHARGOS B 2000 – 2009 programme aims • De-institutionalised mental care delivery in community-based structures and facilities; • Development of an integrated network of primary and acute mental care services • Promotion of illness prevention, social and labour market inclusion • Cost of programme: € 216.2ml (2000); € 255.2mio (2008) • Committed funding: ESF: 182.6ml, ERDF: 21.5ml, national funds: 51.1ml Challenges • Modernisationofphysicalinfrastructure • Development ofprimarycarestructures • Promotion ofpreventivehealthcareandsocialinclusion • Investment strategy: useof national and EU funds • Culture changeandprofessional development
PSYCHARGOS B 2000 – 20009 ProgrammeOutcomes • Closure of asylum wards in 5 psychiatric hospitals, reduction of patients in 5 remaining hospitals: 68% reduction of hospital beds • Operation of new extramural (community-based) care structures for up to 2,050 patients • Operation of 80 employment promotion structures • Training of 3,000 mental care professionals Recommendations • Programme duration of 5 years too short: programme activities are still being pursued in 2011, as part of the 4th programming period of 2007 -13, a spending overhang; • Philanthropy, 3rd sector funding options need to be formally assessed and included in programme design and delivery • Private actor participation needs to be better supported through (i) care quality control framework, (ii) simplified procurement processes • De-institutionalisation may start once community-based care structures, care quality control framework have been established
EIII specific observations (1)(Subject to ongoing thematic analysis) • “Process bureaucracy is process bureaucracy” • Risks of a ‘tick box’ approach • Risks of over-ambition and over-statement • Decisions, but with uncertain accountability - & ownership of ROI • Can be ad-hoc and opportunistic basis for SF proposals • Tendency towards tactical, as opposed to strategic investment • Scale of ‘legacies’ can create overwhelming problems: • Short-term easement of pressures in place of transformational change • Absorption capacity • Political uncertainty
EIII specific observations (2) • Difficulties over integration of projects and programmes - masterplanning weaknesses and implementation problems • E.g. Disconnection - eHealth / Capital Asset provision (handout) • Questionable financial realism & some evidence of over-expectation spirals • In comparison with non-SF and ‘progressive’ health systems – a weakness in visioning, innovation and transformational change • Under-estimation / under-exploitation of the dramatic changes underway in healthcare
Critical success factorsSF investment in future health-care • Accountability – and owning performance and evaluation • Strategic vision and tactical competence • Financial realism • Integrated masterplanning and programming, including investing for continuous change • Accessing (and applying) technology diffusion • Investing for measurable ROI (return on investment) • Population health status • Health outcomes • Economic impact • An understanding of and commitment to social cohesion • The three integrated elements of healthcare delivery: • Service delivery models (disease management and pathways) • Workforce • Capital (infrastructure, technology and ICT)
Why sustained change is critical for EUsocial and economic cohesion The Paradox - substantially enhanced by the economic situation • More progress needs to be made more quickly to reduce inequalities: • Population Health Status • Healthcare Quality e.g. health outcomes, avoidable mortality (a growing factor is the quality of cross border care) • There is also an urgent need for (investment-led) transformational change to reconcile revenue cost and affordability, but: • Capital investment is challenged by debt management / reduction needs • Service investment is threatened by affordability within the volatile and fragile economic climate • PPP presents affordability risk • For the ’12’ in particular, If there is no progress, poor health and the impact of ageing populations will: • Threaten social cohesion, and • Challenge economic growth and stability – impact of the high cost burden • There is a risk that the ’12’ (in particular) will be locked into ongoing legacy problems, which in turn generate fiscal governance problems.