Download
1 / 39
430 likes | 702 Views
Epidemiology of Filariasis. Epidemiology of Filariasis. Magnitude of the problem Life cycle: Agent & Vector Clinical features Diagnosis Treatment. introduction. Caused by the nematode worm either Wuchereria bancrofti or Brugia malayi

E N D
Epidemiology of Filariasis • Magnitude of the problem • Life cycle: Agent & Vector • Clinical features • Diagnosis • Treatment
introduction • Caused by the nematode worm either Wuchereriabancrofti or Brugiamalayi • Transmission: Culexquinquefasciatus & Mansoniaannulifera/uniformis • Lymphatic system is affected • The disease manifests often in bizarre swelling of legs and hydrocele • A great deal of social stigma
introduction • A major public health problem in India • Recorded in “Susruta Samhita” • Clarke called elephantoid legs in Cochin as Malabar legs
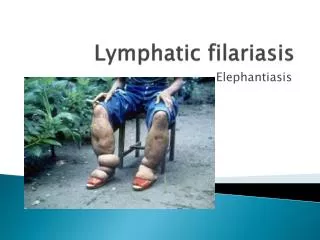
filariasis • Lymphatic filariasis • Wuchereriabancrofti, • Brugiamalayi • Brugiatimori • Lymphatic filariasis • O. Volvulus • M.Ozzardi etc
Magnitude of the problem: global • A major cause of clinical suffering, disability and handicap • Approximately 18% of the world's population — live in areas at risk of infection with lymphatic filarial parasites • Approximately one third of those at risk live in India, one third in Africa
Socio - economic burden • Second leading cause of disability in the world. • Causes stigma, isolation, psychological stress and family discord among the affected individuals • Impairs educational and employment opportunities • Impedes domestic and occupational activities
Socio-economic burden • A male chronic patient on average losses as many as 69 working days/annum • The treatment costs incurred by patients range from RS 1 to 1000 per episode an • India loses also 1.2 billion man days due to LF
Epidemiology of Filariasis • Magnitude of the problem • Life cycle: Agent & Vector • Clinical features • Diagnosis • Treatment
About the vectors • W. bancrofti : Culex mosquitoes in most urban and semi-urban areas • Anopheles in the more rural areas of Africa and • Aedes species in many of the endemic Pacific islands.
The vector • Brugian parasites : Mansonia species serve as the major vector • Brugian parasites are confined to areas of east and south Asia, especially China, India, Indonesia, Malaysia and the Philippines.
Epidemiology of Filariasis • Magnitude of the problem • Life cycle: Agent & Vector • Clinical features • Diagnosis • Treatment
Clinical features • Asymptomatic microfilarimia • Acute manifestations • Chronic obstructive lesions • Occult filariasis: Tropical Pulmonary eosinophilia
lymphoedema grading • Grade I : Mostly pitting oedema; spontaneously reversible on elevation. • Grade II: Mostly non-pitting oedema; not spontaneously reversible on elevation. • Grade III (elephantiasis): Gross increase in volume in a Grade II lymphoedema, with dermatosclerosis and papillomatous lesions.
Bancroftian filariasis • Lymphatic vessels of the male genitalia are most commonly affected • Episodic funiculitis (inflammation of the spermatic cord) epididymitis and orchitis • Hydrocele is the most common sign of chronic bancroftianfilariasis, followed by lymphoedema & elephantiasis
Brugian filariasis • Lymphadenitis: one inguinal lymph node at a time • Lymphangitis • The infected lymph node may become an abscess, ulcerate, and heal with fibrotic scarring • Characteristically, elephantiasis involves the leg below the knee but occasionally it affects the arm below the elbow
Epidemiology of Filariasis • Magnitude of the problem • Life cycle: Agent & Vector • Clinical features • Diagnosis • Treatment
Laboratory Diagnosis • Examining night blood collected by finger pricking • Og4C3 ELISA Assay • ICT Card Test • Polycarbonate membrane filtration Test • Other tests • Serological techniques Indirect immuno fluorescent assay with mf and adult worm. • DNA based diagnostic tests
Epidemiology of Filariasis • Magnitude of the problem • Life cycle: Agent & Vector • Clinical features • Diagnosis • Treatment
Case treatment • Diethylcarbamazine (DEC): 6 mg/kg • For 12 days over 2 weeks • Toxic reactions • Ivermectin : 400 micro gm/kg single dose
lymphoedema management • Washing • Prevention and cure of entry lesions • Elevation of the foot • Exercise • Wearing proper footwear • Hydrocelectomy
Mass Drug Regimen • 6 mg/kg diethylcarbamazine citrate (DEC) + 400 mg albendazole • 150 µg/kg ivermectin + 400 mg albendazole (in the case of co-endemicity with onchocerciasis) • A third option is to follow a treatment regimen using DEC-fortified cooking salt daily for a period of 12 months
questions • Clinical Spectrum of Filariasis • Treatment of Lymphatic Filariasis and Mass treatment regimen.
Next class • Filaria survey • Prevention & control strategies