Download

1 / 33
330 likes | 436 Views
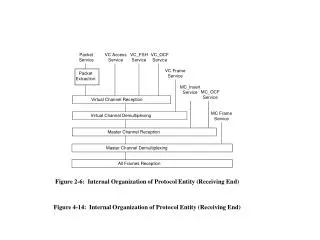
TRAINING PACKET. TABLE OF CONTENTS. Page(s ) Table of Contents ………………………………………………………………..……………………….……….2 Washington State Migrant Health Procedure ……………………………….………...……….… 3-5 Migrant Physical exam and Health Data Reporting Form………………………………………..6

E N D
TABLE OF CONTENTS Page(s) • Table of Contents………………………………………………………………..……………………….……….2 • Washington State Migrant Health Procedure……………………………….………...……….…3-5 • Migrant Physical exam and Health Data Reporting Form………………………………………..6 • Migrant Physical Examination Summary Form………………………………………………….….…7 • Migrant Physical Exams: A Guide for Parents (English & Spanish)…………………………………………………………………………………………………………..….8-9 • Physical Examination Requirements (English & Spanish)………………………………………………………………………………………………………...…...10 • Migrant Physical Examination Check List…………………………..……………………………...…11 • Record of Student Health History (English & Spanish)…………………..…….………………………………………………………………………………12-15 • Parent Interview/Health History (English & Spanish)…………………..…………………………………………………………………………………….…..16 • Current Health Concerns Form……………………………………………………………….…………..17 • Provide the Following Documents if Available.………………………………………………………………………………………..…………..……...18 • Referral Note, Medical (English & Spanish)……………………………………..……………….….19 • Dental Outcomes……………………………..………………………………………………………………....20 • Referral Note, Dental (English & Spanish)………………………..……………………….…...……21 • Form Distribution Protocol…………………….………………….…………………………………………22 • Migrant Dental Screenings (English & Spanish)……………………………..…………………..…23 • Parent Notification of Exam (English & Spanish)…………………………………….……….……24 • Sample Letter to Parents (English & Spanish)………………………………………..…….….25-26 • Screening Room Set-up…………………………………………………………………………………....…27 • Tuberculin Skin Test (TST) Recommendations for Children…………………………………….………………………………………………………………….…….28 • PPD Referral (English & Spanish)………………………………….……………………………….…....29 • Provider Evaluation…………………………..…………………………………………………………..…30-31 • School District Evaluation…………………………………….……………………………………….….…32
WASHINGTON STATE MIGRANT HEALTH PROCEDURE • Rev. 09/07/11 The Health Supervisor provides statewide-required trainings to local education agencies (LEAs) and clinic provider personnel in the physical examination process. • Confirms examination dates with the LEA and the number of students to receive physicals utilizing Migrant Education Program (MEP) funds. • Sets a proposed schedule utilizing the LEA physical exam survey and post schedule on the Migrant Education Health Program (MEHP) website under Physical Exam Dates by MERO to each LEA. Once requested, dates are confirmed by the health provider. • Provides necessary forms for paperwork for examinations to each LEA and health provider. Any ensuing changes in the schedule must be made through the Health Supervisor at 509-682-0373/miket@ncesd.org or the Health Secretary at 509-682-3248/rosemarieh@ncesd.org. The LEA provides the following prior to their physical examination clinic: • Download the Possible Priority for Services (PPFS) Without Exams Report from the Migrant Student Data and Recruitment (MSDR) Migrant Student Information System (MSIS) which identifies PPFS students and students that have not received a physical examination in the last three years. Students are allowed one Title I migrant funded physical examination every three years unless the LEA has a concern, which requires another assessment to determine a problem. Insured students are allowed as many exams as their insurance will allow. • LEAs must serve PPFS students who have not received an exam for three (3) years first. Once those students have been served, you may serve other eligible, current migrant students. • Print on-line copies of student lists as appropriate. • Utilize the electronic Claim/Summary Forms found on the MSIS to develop student lists and electronically submit Summary Forms on line. Print on-line copies of their MSIS transfer document (health record) for the purpose of evaluation. This is attached to the Migrant Physical Exam and Health Data Reporting Form (see handout) to apprise the provider of any existing health problems. The LEA should make a copy for their files. After selecting students, parent/guardian(s) are contacted. Your home visitor or designee accomplishes the following by interviews with the parent/guardians: • Prior to utilizing MEP funds, it is required by the “No Child Left Behind” legislation that all state and local resources must be utilized prior to federal funds. In the area of health, this is state, federal, or personal health insurance or other appropriate resources (see handout). • If a student has had a recent physical examination through state, federal, or personal insurance (document your findings in their MSIS record), the student is not eligible for a MEP funded examination. • If the student has state, federal or personal insurance but the parent/guardian if for any reason is unable to have the student assessed, then the LEA acquires a photo copy of the insurance card and includes the student in LEA’s physical examination clinic. • Eligible students without insurance or insurance coverage will have physical examinations funded through the MEP. • Students and parent/guardians have the right to refuse all or any part of a physical examination. Indicate on Migrant Physical Exam and Health Data Reporting Form all screenings/tests refused by parent/guardians and/or student. • Every effort should be made to have parent/guardian(s) present during examinations.
Once you have made your final selection, your staff must complete the following prior to the health provider’s assessment: • Completes non-shaded sections of the Migrant Physical Exam and Health Data Reporting Form. • Current height, weight, vision, and hearing screenings completed and noted on the Migrant Physical Exam and Health Data Reporting Form (provider will determine if height and weight are normal, abnormal, or undetermined). • LEA staff will review the MSIS Transfer document and other available student records to determine any health-related concerns that the provider should be apprised of. The home visitor or designee interviews parent/guardians to gather most recent health profile data to obtain the following: health history, does student have a medical home and/or insurance, has the student had an exam in the past three (3) years. If a health concern is identified, it is noted on the Medically Diagnosed Alert Conditions Section of the Migrant Physical Exam and Health Data Form. Complete the electronic Parent/guardian Permission to Examine and Authorization for Release of Information forms and ensures that they are reviewed and signed by the parent/guardian/guardian (see handout). • Completes the electronic Migrant Physical Examination Summary Form(s) at least two weeks prior to clinic date. This is located in the MSIS. • Ensures that any questions from parent/guardians regarding the student's physical status are communicated to the provider, as appropriate. • Has student on site and ready for examination. The Clinic Providers review the student's medical charts, if the student is a clinic patient. The clinic provider informs the LEA if the student recently had a complete physical. The LEA enters this in the student’s MSIS health record. • Performs screens/labs and provides physical examinations as contracted. • Screens records for any unresolved health problems and addresses these during physical examination. • Completes all shaded areas of the Physical Examination Form as contracted. Enters PPD batch data on the electronic Summary Form. • Notes health care problems by checking ( ) shaded side of the MEDICALLY DIAGNOSED ALERT CONDITIONS Section, ICD Codes; refers student for follow-up care as appropriate. Determines if height and weight are normal, abnormal, or undetermined. • Notes in the Health Profile if the physical exam is normal or abnormal. • Notes results in the HEALTH PROFILE Section as normal, abnormal, or undetermined which are indicated for each problem; refers student for follow-up care as appropriate. • The Migrant Physical Exam and Health Data Reporting Form is signed by the examiner at the conclusion of the examination (or examination day). • Indicates on all copies of the Migrant Physical Exam and Health Data Reporting Form all tests refused. • Gives pink copy of Physical Examination Form to LEA on examination day for MSIS inputting and takes remaining three copies. • Discusses necessary follow-up and referrals with migrant LEA staff after examinations are completed each day. • Fills out Referral Forms, as appropriate.
The LEA: • Informs parent/guardians of examination results and assists in obtaining follow-up care, where necessary. • Assists parent/guardians in obtaining insurance through state or federal program services (see handout). • Reads PPDs within 48-72 hours and records in millimeters induration on the Electronic Physical Examination Summary Form within one week. • Refers students with positive or questionable PPD results to local county health department or primary care provider as appropriate. • Records clerk or designee inputs physical examination data into the MSIS. • Completes Physical Examination Evaluation of Health Provider Form and submits to Health Supervisor. • The Clinic Provider: • Records PPD results on the Migrant Physical Exam and Health Data Reporting Form. • Submits the yellow and goldenrod ESD copies of the Migrant Physical Exam and Health Data Reporting Forms to the Health Supervisor and electronically submits the ESD Service Claim Form within 30 days. • Completes Migrant Physical Evaluation Form of LEA and submits to Health Supervisor. • The Health Supervisor: • Reviews Migrant Physical Exam and Health Data Reporting Forms and Service Claim Forms for accuracy and completeness. When approved, the Health Supervisor will submit the claim to the ESD fiscal office for payment. • Returns any incomplete forms or contacts clinic for information before payment is approved.
PHYSICAL EXAMINATION REQUIREMENTS ELIGIBILITY/PRIORITY Eligibility for students’ physical examinations is based on meeting the following criteria: • The parent(s)’ consent has been obtained on the Certificate of Eligibility (COE) for the physical examination. Parent and/or student may elect to decline any or all parts of the physical examination. • The student has been enrolled in the Migrant Student Data and Recruitment Office (MSDR). • All state, federal, and personal medical insurance resources must be pursued prior to the utilization of Title I Migrant Education funds. • Priority for physical examinations is given to migrant students who have not received a physical examination for three years, or have a current health concern. • Note: The Office of Superintendent of Public Instruction, Migrant Education Program, requires the inclusion of health services. Health data is reviewed to ensure completeness and accuracy. REQUISITOS PARA UN EXAMEN FISICO PRIORIDAD/ELELEGIBLE Los requisitos para que un estudiante reciba un examen físico se basan en la siguiente criterio. • Para un examen físico se ha obtenido el consentimiento de los padres en el certificado de elegibilidad (COE). Los padres y/o el estudiante pueden evadir una o todas las partes del examen físico. • Que el estudiante sea registrado en la Oficina de Datos y Reclutamiento para Estudiantes Migratorios (MSDR). • Se deben utilizar todos los recursos necesarios, los del Estado, Federal y a seguranzas médicas personales, antes de utilizar los fondos del Programa del Título I de Educación Migrante. • A los estudiantes migrantes se les da prioridad para recibir un examen médico, si no han tenido uno por un lapso de tres años, y/o tienen algún problema de salud inmediato. Nota: La oficina del Superintendente de la Instrucción Pública y el Programa de Educación Migrante, solicitan que se incluyan servicios de salud. Las estadísticas son revisadas continuamente para asegurarse de su competencia y precisión.
RECORD OF STUDENT HEALTH HISTORY Student Number: / / / / / / / / Student Name: Last First MI Birthdate: / / / Please indicate with a check mark in the appropriate column whether the child has had the illnesses listed below. T
ESPEDIENTE DE LA SALUD MEDICA DEL ESTUDIANTE Numero del Estudiante: / / / / / / / / /Fecha de Nacimiento: / / / Nombre del Estudiante:Apellido Primer NombreInicial En la columnaapropiadapor favor marque lasenfermedadesque ha tenido el estudiante. T
Parent Interview/ Entrevista de Padres de Familia Student’s NameDate of Birth: / / / Nombrede EstudianteFecha de Nacimiento: / / / MSDR NumberNúmero del MSDR: Does your child have a doctor? Yes No ¿Tiene su hijo(a) un doctor? Si No If yes, who? Si surespuestaes Si, Quién es? Has yourchildrecentlyhad a physicaleamination? Nameof doctor seenlastyear? ¿Ha tenido su hijo(a) un examen físico recientemente? Nombre del doctor que vio el año pasado? Doesyourchildhave a dentist? Yes No ¿Tiene su hijo(a) un dentista? Si No If yes, who? Nameof dentistseenlastyear? Si surespuestaes Si, Quién es? Nombre del dentista que vio el año pasado Has yourchildrecentlyhad a dental examination? (Within 6 monthsto 1 year) Yes No ¿Ha tenido su hijo(a) un examen dental recientemente? (Entre seis meses a un año) Si No Doesyourchildhave medical insurance? Yes No ¿Tiene su hijo(1 seguro Médico/asequranza? Yes No PrivateInsurance Seguro Privado Medicaid: Citizenor non-citizen) (ciudadano y no ciudadanos) Children’sHealthInsuranceProgram (CHIPS) Basic HealthProgram (ifstudentis 19 orolder) (si el estudiante es mayor de ó tiene 19 años) Do youwantyourchildtohave a physicalexamination at schoolprovidedbythe Migrant Education Program at no costtoyou? Yes No ¿Le gustaría que su hijo(a) tuviera un examen físico en la escuela, proveido gratuitamente por el Programa de Educación Migrante? Si No
CURRENT HEALTH CONCERNS FORM StudentBirthdate Last/First/Middle Month/Day/Year MSDR No. Health Concern Reporter's Name School District Reporter's Position
PROVIDE THE FOLLOWING DOCUMENTS IF AVAILABLE • Transfer document (health record) • Immunization Record • Current Health Concern Form • Only if you have knowledge of a problem the provider should address • Insurance card • If the student has coverage, if not, you should assist the family with the acquisition of services
FORM DISTRIBUTION PROTOCOL At the conclusion of each clinic, the Migrant Physical Examination Form and Referral Forms need to be separated. The following protocol will assist you in this task. MIGRANT PHYSICAL EXAMINATION FORMS: Provider – white, goldenrod, and yellow School District – pink REFERRAL FORMS: Provider – white and goldenrod School District – pink and yellow PROCEDURE: Provider retains the white Physical Examination Form and Referral Form copy for files. Provider submits the following to ESD: yellow and goldenrod copy of Examination Form, goldenrod copy of Referral Form, along with billing and itemized list of students examined during clinic. School retains pink copy of Physical Examination Form and Referral Form for district files. School routes yellow copy of Referral Form to parents for follow-up care. DENTAL OUTCOMES: Provider retains white copy for files. Providersubmits yellow copy to ESD. T School retains pink copy for district files.
Migrant Dental Screenings Child’s Last Name First NameMI Date of Birth(month/day/year) Sex: MF AddressCity StateZipTelephone ( ) - Please Circle All that Apply: Yes, I want my child to have a Dental Screening Yes, I also want my child to have a Fluoride treatment No, I do not want my child to have a Dental Screening or Fluoride If your child has other treatment needs we will contact you to try to schedule a follow up visit. A parent or guardian must be present at that follow up visit in order to do any dental procedures. Signature of Parent or Legal GuardianDate ************************************************************************ ApellidoNombreMI Fechade Nacimiento(Mes/Día/Ano) Sexo: MF DirecciónCiudad EstadoCódigo PostalTeléfono( ) - Porfavormarque lo pertinente: Si, Yoquieroque me niño/a obtanga un chequeo dental (realizadopor dentist o higienista) Si,Yoquieroque mi niño/a obtengatratmiento de fluoruro No, Yo no quieroque me niño/a obtengaun chequeo dental e fluoruro Si suniñonecesitatratamientoadicionalnoscomunicaremos con ustedparahacerunacita de seguimiento. Un padre?madre/tutor necesitaráacompañar el/la niño/a a la citaparaobtenerserviciosdentales. Firma Padre/Madre o TutorFecha
PARENT NOTIFICATION OF EXAM Dear Parent: Your child has been scheduled for a migrant student physical examination on . This examination is provided at no cost to you. date You are invited and encouraged to attend your child’s examination. If you do plan to attend, please contact name at , so we can phone number, school name ensure that your child receives his/her exam while you are present. Sincerely, ************************************************************ Estimado(a) Padre/Madre: Su hijo(a) tieneunacitapara un examenfísicoparaestudiantesmigrantes el . Este examenesproveído a ninguncosto fecha parausted. Se le invita y se le anima a queasista a la examinación de suhijo(a). Si ustedpiensaatender, y paraasegurarquesuhijo(a) receiba el examen en supresencia, haga el favor de comunicarse con (nombre) al número en . nombre do escuela Sinceramente,
* * * * SAMPLE LETTER TO PARENTS * * * * * IMPORTANT NOTICE Dear : This letter is to inform you that your son/daughter, , received a physical examination on at . These services were provided through the Migrant Education Program. It is important that you keep this document with your child’s permanent health records. The findings from the examination are as follows: Your child was found to be in satisfactory health Anemia Ear infection Excessive earwax Undescended testicles Positive T.B. test Heart murmur Failed vision screening Failed hearing screening Cavities Throat infection Urinary tract infection Warts Obesity Elevated blood pressure Acne Short stature Other The doctor recommended that your son/daughter be scheduled for an appointment with your family physician or a doctor of your choice. The following are health resources available that offer reduced cost or sliding fee scale according to your income.
* * * * MUESTRA: CARTA A PADRES DE FAMILIA * * * * * EN LOS DISTRITOS ESCOLARES AVISO IMPORTANTE Estimado(a) Sra. : Esta carta es para infórmale de que su hijo(a) , recibió un examen medico el día localizado en . Estos servicios fueron proveídos por medio del programa Educación Migrante. Es importante que Ud. Mantenga este documento junto con los documentos médicos permanentes de su hijo(a). Los resultandos del examen son los siguientes: Su hijo(a) está en buena salud Su hijo(a) padece de anemia Su hijo(a) padece de infección del oído Su hijo(a) padece de cerumen (cera en los oídos) excesivo Su hijo padece de criptorquidia (defecto de posición de los testículos) El resultado del examen tiene indicaciones positivas de tuberculosis Su hijo(a) padece de rumor cardiaco Su hijo(a) fallo en la prueba de audición Su hijo(a) fallo en la prueba de vista Su hijo(a) tiene problemas dentales Su hijo(a) padece de infección de la garganta Su hijo(a) padece de infección urinaria Su hijo(a) padece de verrugas Su hijo(a) padece de obesidad Su hijo(a) padece de presión elevada Su hijo(a) padece de acné Su hijo(a) padece de estatura baja Su hijo(a) padece de otro problema El médico recomienda que Ud. Haga una cita para su hijo(a) cónsul médico familiar, o un médico de su elección. La siguiente es una lista de agencies que proveen servicios médicos a base de cobros reducidos o cobros variables basados en los ingresos familiares.
Bed Desk SCREENING ROOM SET-UP One Provider Team * Electrical Outlet Chair Chair Waste Basket • Room must afford complete privacy • Bathroom in room or in close proximity • Waiting area • Optional: Table with crayons and coloring books for waiting children. Chairs for parents. Two or More Provider Team Screen * Electrical Outlet Chair Chair Waste Basket Table Bed Desk Table
PPD REFERRAL DateMSDR NameBirthdate Address Directions Parent's Names Date PPD GivenResults (in mm) PPD Given ByPPD Read By School NameSchool District Contact Person Refer to your local health department if PPD results are 5 mm or greater of induration. Please bring this referral sheet. Child must be accompanied by a parent. ****************************************************************************** PPD REFERRAL FechaMSDR NombreFecha de Nacimiento Domicilio Instrucciónesparaalcanzar el domicilio Nombre de padres Fecha de PPDResultados (en mm) PPD dado porPPD leidopor Nombrede la escuelaDistrito Escolar Dirección de la escuela Persona de contactar Favor de reportar a sudepartamento local de saludsi los resultados de PPD indican 5 mm o mas de induración. Favor de traeresta forma. El padre debe de estar con el niño.
WASHINGTON STATE SCHOOL DISTRICT MIGRANT PHYSICAL EXAMINATION OF PROVIDER EVALUATION Date 1. Were physicals conducted at an appropriate time of year/date, taking impaction period into consideration, and school district preferred dates as submitted to the Health Supervisor? YesNo Comments: 2. Did provider arrive at school sites at the scheduled time? Yes___ No ___ Comments: 3. Did provider spend a minimum of 10 minutes per child, hands-on physical examination (excluding lab and paperwork)? A maximum of five (5) children per hour should be examined. Yes ___ No ___ Comments: • Was the necessary paperwork completed at the appropriate time? YesNo Comments: 5. Did provider meet with school staff to review any existing or unresolved health problems on the child's health record? Yes ___ No ___ Comments: 6. Did you encounter any difficulties in the scheduling and delivery of physical examinations? If so, please comment. Yes ___ No ___ Comments: 7. Were parents encouraged to be present at examinations or to volunteer at the examination site? Yes ___ No ___ Comments: OVER
Evaluation Form • Page 2 • 8. Was time allowed for debriefing and providing information or referrals? Yes ___ No ___ • Comments: • 9. In your opinion, what can be done to improve the health examination procedure or quality of examination? • Comments: • 10. How do you rate this year's physical examination? • Low High • Process: 1 2 3 4 5 6 7 8 9 10 • Quality of Examination: 1 2 3 4 5 6 7 8 9 10 • Evaluation results will be compiled by the Migrant Health State Supervisor and shared at next year's contract renewal meeting. • Evaluation by: • Name/Title: • School District: Date • Please return to: Mike Taylor, Migrant Health State Supervisor • North Central ESD • P.O. Box 2424 • Chelan, WA 98816 • (509) 682-0373/miket@ncesd.org FAX (509) 682-3407 or (509) 682-3248/rosemarieh@ncesd.org
WASHINGTON STATE PROVIDER MIGRANT PHYSICAL EXAMINATION EVALUATION OF LEA DATE 1. Did the LEA provide adequate facilities for the physical exams? Yes ___ No ___ Comments: 2. Did the LEA complete the appropriate paperwork for providers and was the MSDR health record attached for each student? Yes ___ No ___ Comments: 3. Did LEA staff meet with the provider to review any health problems that are classified as unresolved in health records as any existing health problems or parental concerns? Yes ___ No ___ Comments: 4. What in your opinion would improve the health examination process? Comments: 5. Were PPDs recorded and information returned to the clinic on time? Yes ___ No ___ Comments: 6. How do you rate this year's physical examination? LowHigh Process: 1 2 3 4 5 6 7 8 9 10 Quality of Examination: 1 2 3 4 5 6 7 8 9 10 Evaluation results will be compiled by the Migrant Health State Supervisor and shared at next year's contract renewal meeting. School District: Clinic Name: Prepared By: Phone Number: Please return to: Mike Taylor, Migrant Health State Supervisor North Central ESD P.O. Box 2424 Chelan, WA 98816 (509) 682-0373/fax 682-3407/miket@ncesd.org