Download
1 / 1
10 likes | 113 Views
G.A. Tramper-Stranders 1 , C.K. van der Ent 1 , A. Fleer 3 , J.L.L. Kimpen 2 , T.F.W. Wolfs 2 1 Department of Paediatric Respiratory Medicine 2 Department of Paediatric Infectious Diseases 3 Department of Medical Microbiology

E N D
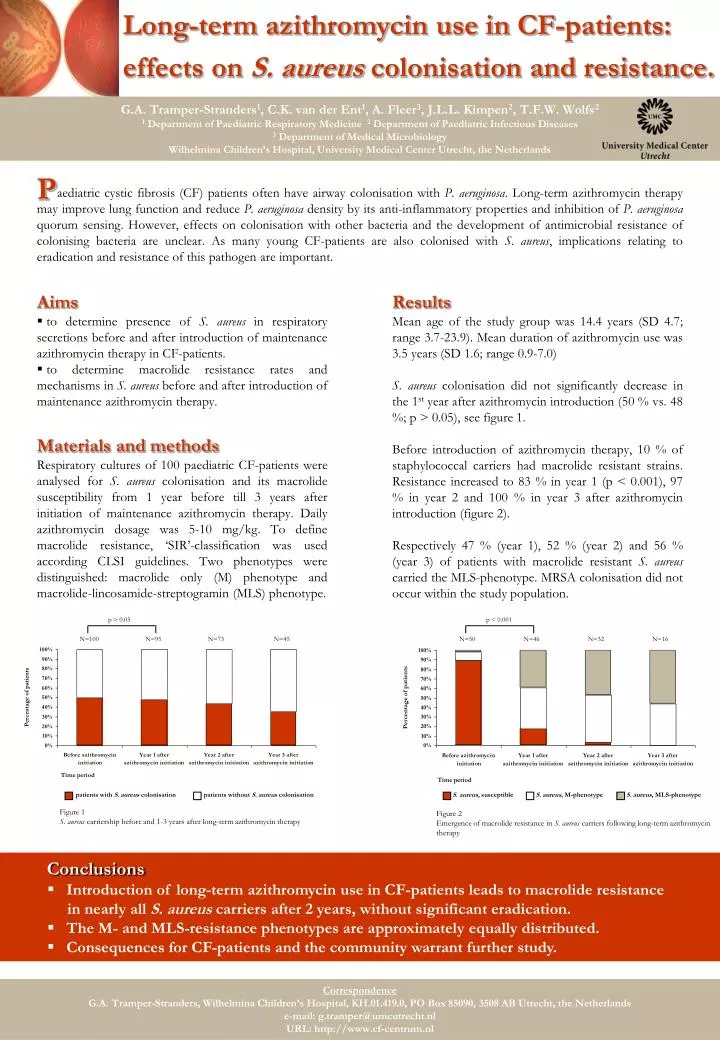
G.A. Tramper-Stranders1, C.K. van der Ent1, A. Fleer3, J.L.L. Kimpen2, T.F.W. Wolfs2 1 Department of Paediatric Respiratory Medicine 2 Department of Paediatric Infectious Diseases 3 Department of Medical Microbiology Wilhelmina Children’s Hospital, University Medical Center Utrecht, the Netherlands P Long-term azithromycin use in CF-patients: effects on S. aureus colonisation and resistance. aediatric cystic fibrosis (CF) patients often have airway colonisation with P. aeruginosa. Long-term azithromycin therapy may improve lung function and reduce P. aeruginosa density by its anti-inflammatory properties and inhibition of P.aeruginosa quorum sensing. However, effects on colonisation with other bacteria and the development of antimicrobial resistance of colonising bacteria are unclear. As many young CF-patients are also colonised with S. aureus, implications relating to eradication and resistance of this pathogen are important. Aims Results • to determine presence of S. aureus in respiratory secretions before and after introduction of maintenance azithromycin therapy in CF-patients. • to determine macrolide resistance rates and mechanisms in S. aureus before and after introduction of maintenance azithromycin therapy. Mean age of the study group was 14.4 years (SD 4.7; range 3.7-23.9). Mean duration of azithromycin use was 3.5 years (SD 1.6; range 0.9-7.0) S. aureus colonisation did not significantly decrease in the 1st year after azithromycin introduction (50 % vs. 48 %; p > 0.05), see figure 1. Before introduction of azithromycin therapy, 10 % of staphylococcal carriers had macrolide resistant strains. Resistance increased to 83 % in year 1 (p < 0.001), 97 % in year 2 and 100 % in year 3 after azithromycin introduction (figure 2). Respectively 47 % (year 1), 52 % (year 2) and 56 % (year 3) of patients with macrolide resistant S. aureus carried the MLS-phenotype. MRSA colonisation did not occur within the study population. Materials and methods Respiratory cultures of 100 paediatric CF-patients were analysed for S. aureus colonisation and its macrolide susceptibility from 1 year before till 3 years after initiation of maintenance azithromycin therapy. Daily azithromycin dosage was 5-10 mg/kg. To define macrolide resistance, ‘SIR’-classification was used according CLSI guidelines. Two phenotypes were distinguished: macrolide only (M) phenotype and macrolide-lincosamide-streptogramin (MLS) phenotype. p > 0.05 p < 0.001 N=100 N=95 N=73 N=45 N=50 N=46 N=32 N=16 patients with S. aureus colonisation patients without S. aureus colonisation Figure 1 S. aureus carriership before and 1-3 years after long-term azithromycin therapy S. aureus, susceptible S. aureus, M-phenotype S. aureus, MLS-phenotype Figure 2 Emergence of macrolide resistance in S. aureus carriers following long-term azithromycin therapy • Conclusions • Introduction of long-term azithromycin use in CF-patients leads to macrolide resistance in nearly all S. aureus carriers after 2 years, without significant eradication. • The M- and MLS-resistance phenotypes are approximately equally distributed. • Consequences for CF-patients and the community warrant further study. Correspondence G.A. Tramper-Stranders, Wilhelmina Children’s Hospital, KH.01.419.0, PO Box 85090, 3508 AB Utrecht, the Netherlands e-mail: g.tramper@umcutrecht.nl URL: http://www.cf-centrum.nl