Download
1 / 50
510 likes | 723 Views
Vaginal Infections and Preterm Birth - An Update. J. Chris Carey, MD. Disponible en: http://www.ihs.gov/MedicalPrograms/MCH/M/documents/VIPPRES2.PPT. History Rationale Asymptomatic bacteriuria Gonorrhea Syphilis Genital Mycoplasmas. Chlamydia trachomatis Group B strep

E N D
Vaginal Infections and Preterm Birth -An Update J. Chris Carey, MD Disponible en: http://www.ihs.gov/MedicalPrograms/MCH/M/documents/VIPPRES2.PPT
History Rationale Asymptomatic bacteriuria Gonorrhea Syphilis Genital Mycoplasmas Chlamydia trachomatis Group B strep Periodontal disease Bacterial vaginosis Trichomonas vaginalis Overview
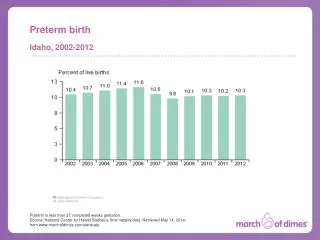
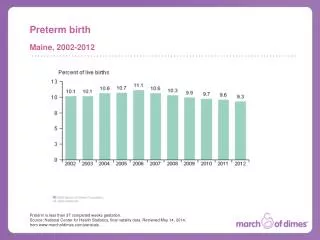
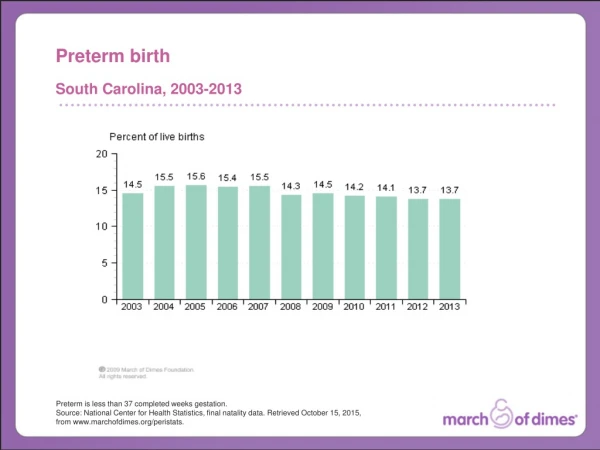
Rationale • Preterm birth is the leading cause of neonatal morbidity and mortality • Increasing body of evidence to indicate that infections are associated with preterm birth
Evidence linking infection with preterm birth • Histologic Chorioamnionitis is more common in preterm deliveries • Postpartum endomyometritis (PPE) is more common after preterm deliveries • Preterm delivery is more common in women with a variety of genital infections
Asymptomatic bacteriuria • Occurs in 3 - 10 % of pregnant women • First asymptomatic infection to be linked to preterm birth
Asymptomatic bacteriuria • Kass (NY State J Med 1962:62: 2815) showed • 24% preterm birth in untreated • 10% in treated • 10% in controls
Asymptomatic bacteriuria • Screen all women at first visit • Treatment reduces risk of pyelonephritis
Syphilis • Effects of untreated syphilis include stillbirth, preterm birth and congenital anomalies • Half of congenital syphilis occurs in women with no prenatal care • Screen all pregnant women at first visit – high risk in third trimester
Gonorrhea • Occurs in 1 - 6 % of pregnant women • Untreated gonorrhea associated with preterm delivery and PPROM • Treatment of gonorrhea reduces risk
Genital Mycoplasmas • Ureaplasma urealyticum • Found in 50 - 90% of pregnant women • Early studies indicated strong association with preterm birth • Later studies fail to confirm association
Ureaplasma treatment trial - VIP • 1181 women - 605 erythromycin, 576 placebo • No difference in • mean birth weight • low birth weight • delivery < 37 weeks • delivery < 32 weeks
Genital Mycoplasmas • Mycoplasma hominis • Inconclusive results from studies • ¿ Association with BV ?
Chlamydia trachomatis • Early studies showed a strong association with preterm delivery and neonatal death • Later studies show an association with preterm delivery and low birth weight • Treatment trials are inconclusive
Group B strep • Early studies showed association between early onset GBS sepsis and preterm birth • Early studies also showed association between preterm birth and GBS carriage • Large study showed weak association • Treatment trials showed no effect of therapy
Group B Strep • VIP study results • GBS recovered from 21 % of 13,646 women • Heavy colonization was associated with a modest risk of preterm low birth weight infant (RR 1.5, 95% CI 1.1-1.9 ) • Light colonization showed no increase risk • Treatment with antibiotics active against GBS reduced risk in heavily colonized women • Regan et al AJOG 1996;174:1354-60
Group B Strep • VIP study • Randomized clinical trial of erythromycin did not reduce the risk of preterm birth in women colonized with GBS
Bacterial vaginosis • Occurs in 20 – 30 % of asymptomatic women • Approximately 1,000,000 cases/yr in USA in pregnant women • Numerous studies show association with preterm birth
Bacterial vaginosis • Gravett, 1986 JAMA • N=534 pregnant women (102 with BV) • BV associated with • PROM (RR= 2.4) • Preterm labor (RR = 2.0) • IAI (RR = 2.7)
Bacterial vaginosis • Kurki - Obstet Gynecol 1992 • N = 790 pregnant women • BV by culture 21.4% • BV by Gram stain 21.1% • BV associated with • PTL RR 2.6 • PTB RR 6.9 • PPROM RR 7.3
Bacterial Vaginosis • Hay – BMJ 1994 • N=783, screened at 9-24 weeks • BV associated with • PTD – RR 2.8 • Late miscarriage – 5.5
Bacterial vaginosis • Total of 11 studies show increase in PTB with RR ranging from 2 - 4
Bacterial vaginosis • VIP data – Hillier NEJM 1995 • N = 10,397 women without chlamydia, TV or GBS • BV in 1645 • PTD – rr 1.4 • LBW – rr 1.5
BV treatment trials • Clindamycin trials • McGregor AJOG 1994 • Joesoef AJOG 1995 • Metronidazole trials • Morales AJOG 1994 • McDonald et al - Br J Obstet Gyn 1997;104:1391
Treatment of BVHauth NEJM 1995 • 263 high-risk women with BV • Randomized 2:1 metro + erythro or placebo • Incidence of PTD • < 37 w - 37% v 23% • < 34 w - 19% v 11% • < 32 w - 11% v 6%
McDonald BV trial • 879 women with BV by Gram stain or culture for G Vaginalis at 19 weeks • Oral metronidazole 400 mg BID for 2 days or placebo at 24 weeks and at 29 weeks if persistent
MFMU BV StudyNEJM 2000 • Purpose – To determine whether treatment of BV with metronidazole would prevent preterm birth • Screened from 8-22 weeks • Treated with 2 grams metro on day 1 and 3 from 13 – 24 weeks • Treatment repeated late second trimester
MFMU Trichomonas trial • Carriage of T. vaginalis increases risk of preterm birth • T. vaginalis commonly found with BV • T. vaginalis is common and often asymptomatic
Purpose • To determine if metronidazole treatment would prevent preterm birth in asymptomatic women who carried T. vaginalis
Randomized • 297 patients randomized to placebo • 320 randomized to metronidazole • The study was stopped early by the Data Safety Monitoring Board
What can we learn from the treatment trials of BV? • Treatment of women with a prior PTD with metronidazole and erythromycin may reduce the risk of subsequent PTD but does not reduce the risk in women who do not have BV • Women with a prior PTD may be in some way different
What should we do in clinical practice? • Screen and treat for gonorrhea, syphilis, asymptomatic bacteriuria, chlamydia • Screen women with a prior PTD for BV and treat with metronidazole and erythromycin? • DO NOT treat BV with clindamycin vaginal cream • DO NOT treat asymptomatic trich
Conclusions • The more we learn, the less we know about infections and preterm delivery • Antibiotic therapy in pregnancy may be harmful • Treatment of infections in pregnancy should only be done if clear benefit has been shown from randomized trials