Download
1 / 1
10 likes | 122 Views
Depression and anxiety in children with epilepsy: Differences in observed and reported levels among parents and children with epilepsy. Trobliger, R., Myers, L., and Lancman, M. Northeast Regional Epilepsy Group, Hackensack, NJ, USA. Introduction

E N D
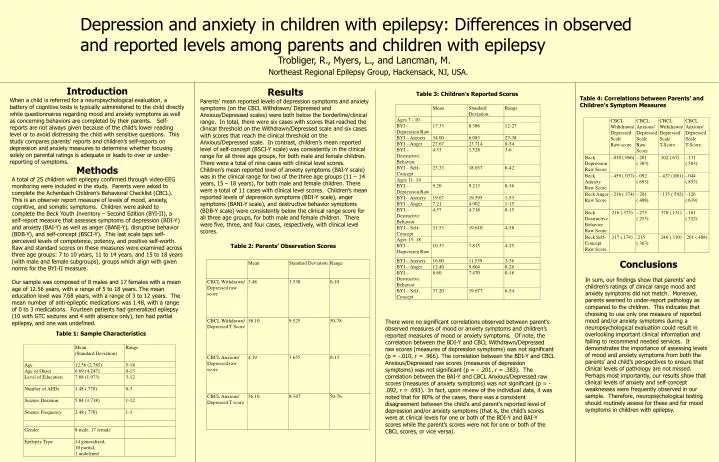
Depression and anxiety in children with epilepsy: Differences in observed and reported levels among parents and children with epilepsy Trobliger, R., Myers, L., and Lancman, M. Northeast Regional Epilepsy Group, Hackensack, NJ, USA. • Introduction • When a child is referred for a neuropsychological evaluation, a battery of cognitive tests is typically administered to the child directly while questionnaires regarding mood and anxiety symptoms as well as concerning behaviors are completed by their parents. Self-reports are not always given because of the child’s lower reading level or to avoid distressing the child with sensitive questions. This study compares parents’ reports and children’s self-reports on depression and anxiety measures to determine whether focusing solely on parental ratings is adequate or leads to over or under-reporting of symptoms. Results Parents’ mean reported levels of depression symptoms and anxiety symptoms (on the CBCL Withdrawn/ Depressed and Anxious/Depressed scales) were both below the borderline/clinical range. In total, there were six cases with scores that reached the clinical threshold on the Withdrawn/Depressed scale and six cases with scores that reach the clinical threshold on the Anxious/Depressed scale. In contrast, children’s mean reported level of self-concept (BSCI-Y scale) was consistently in the clinical range for all three age groups, for both male and female children. There were a total of nine cases with clinical level scores. Children’s mean reported level of anxiety symptoms (BAI-Y scale) was in the clinical range for two of the three age groups (11 – 14 years, 15 – 18 years), for both male and female children. There were a total of 11 cases with clinical level scores. Children’s mean reported levels of depression symptoms (BDI-Y scale), anger symptoms (BANI-Y scale), and destructive behavior symptoms (BDB-Y scale) were consistently below the clinical range score for all three age groups, for both male and female children. There were five, three, and four cases, respectively, with clinical level scores. Table 3: Children’s Reported Scores Table 4: Correlations between Parents’ and Children’s Symptom Measures • Methods • A total of 25 children with epilepsy confirmed through video-EEG monitoring were included in the study. Parents were asked to complete the Achenbach Children’s Behavioral Checklist (CBCL). This is an observer report measure of levels of mood, anxiety, cognitive, and somatic symptoms. Children were asked to complete the Beck Youth Inventory – Second Edition (BYI-II), a self-report measure that assesses symptoms of depression (BDI-Y) and anxiety (BAI-Y) as well as anger (BANI-Y), disruptive behavior (BDB-Y), and self-concept (BSCI-Y). This last scale taps self-perceived levels of competence, potency, and positive self-worth. Raw and standard scores on these measures were examined across three age groups: 7 to 10 years, 11 to 14 years, and 15 to 18 years (with male and female subgroups), groups which align with given norms for the BYI-II measure. • Our sample was composed of 8 males and 17 females with a mean age of 12.56 years, with a range of 5 to 18 years. The mean education level was 7.68 years, with a range of 3 to 12 years. The mean number of anti-epileptic medications was 1.48, with a range of 0 to 3 medications. Fourteen patients had generalized epilepsy (10 with GTC seizures and 4 with absence only), ten had partial epilepsy, and one was undefined. Table 2: Parents’ Observation Scores Conclusions In sum, our findings show that parents’ and children’s ratings of clinical range mood and anxiety symptoms did not match. Moreover, parents seemed to under-report pathology as compared to the children. This indicates that choosing to use only one measure of reported mood and/or anxiety symptoms during a neuropsychological evaluation could result in overlooking important clinical information and failing to recommend needed services. It demonstrates the importance of assessing levels of mood and anxiety symptoms from both the parents’ and child’s perspectives to ensure that clinical levels of pathology are not missed. Perhaps most importantly, our results show that clinical levels of anxiety and self-concept weaknesses were frequently observed in our sample. Therefore, neuropsychological testing should routinely assess for these and for mood symptoms in children with epilepsy. There were no significant correlations observed between parent’s observed measures of mood or anxiety symptoms and children’s reported measures of mood or anxiety symptoms. Of note, the correlation between the BDI-Y and CBCL Withdrawn/Depressed raw scores (measures of depression symptoms) was not significant (p = -.010, r = .966). The correlation between the BDI-Y and CBCL Anxious/Depressed raw scores (measures of depression symptoms) was not significant (p = - .201, r = .383). The correlation between the BAI-Y and CBCL Anxious/Depressed raw scores (measures of anxiety symptoms) was not significant (p = - .092, r = .693). In fact, upon review of the individual data, it was noted that for 80% of the cases, there was a consistent disagreement between the child's and parent's reported level of depression and/or anxiety symptoms (that is, the child’s scores were at clinical levels for one or both of the BDI-Y and BAI-Y scores while the parent’s scores were not for one or both of the CBCL scores, or vice versa). Table 1: Sample Characteristics






