Download
1 / 92
970 likes | 1.46k Views
ECHOCARDIOGRAPHY IN MITRAL STENOSIS. Dr RAJESH K F. CAUSES AND ANATOMIC PRESENTATION. Rheumatic Commissural fusion Leaflet thickening Chordal shortening and fusion Superimposed calcification Degenerative MS Annular calcification Rarely leaflet thickening and calcification at base.

E N D
ECHOCARDIOGRAPHY IN MITRAL STENOSIS Dr RAJESH K F
CAUSES AND ANATOMIC PRESENTATION Rheumatic Commissural fusion Leaflet thickening Chordal shortening and fusion Superimposed calcification Degenerative MS Annular calcification Rarely leaflet thickening and calcification at base
Congenital MS Subvalvular apparatus abnormalities Inflammatory-SLE Infiltrative Carcinoid heart disease Drug induced valve disease Leaflet thickening and restriction Rarely commissural fusion
2D ECHO Commissural fusion PSAX echo scanning of valve Important in distinguishing degenerative from rheumatic valve Complete fusion indicate severe MS Narrow diastolic opening of valve leaflets
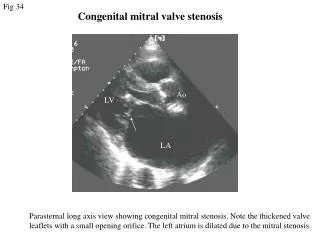
Restricted mobility -PLAX Early diastolic doming motion of the AML- restriction of tip motion
Dilated LA LA and LA appendage thrombus Paradoxical septal motion Dilated RV and RA
Wilkins score -Mitral valve score <8 are excellent candidates for BMV
Limitations of wilkin score Assessment of commissural involvement is not included Limited in ability to differentiate nodular fibrosis from calcification. Doesn’t account for uneven distribution of pathologic abnormalities. Frequent underestimation of subvalvular disease. Doesn’t use results from TEE or 3D echo
3D ECHO TEE and TTE Higher accuracy than 2D echo Detailed information of commissural fusion and subvalvular involvement MVA measurement in calcified and irregular valve MVA measurement after BMV Restenosis after commissurotomy commissural refusion valve rigidity with persistent commissural opening
From LA From LV
Total RT3DE score ranging from 0 to 31 points Total score of mild MV involvement was defined as <8 points Moderate MV involvement 8–13 Severe MV involvement >14
M MODE ECHO Decreased E-F Slope >80 mm/s MVA=4-6cm² <15mm/s⇒ MVA <1.3cm² Thickened Mitral Leaflets Anterior Motion or Immobility of Posterior Mitral Leaflet-tethering at tips Diastolic Posterior Motion of Ventricular Septum (severity of stenosis)
TEE For diagnosis and quantification little yield Spontaneous echo contrast LA and LA appendage thrombus Use of transgastric plane 90 -1200 for evaluation of chordal structures Assessment of commissural calcification and fusion to predict procedural outcome after BMV
Scores for anterolateral and posteromedial commissures were combined such that each valve had an overall commissure score ranging from 0–4 A high score indicated extensively fused, non‐calcified commissures that were therefore more likely to split A low score indicated either minimal fusion or the presence of resistant commissural calcification
ASSESSMENT OF MS SEVERITY 2D OR 3D ECHO MVA BY PLANIMETRY DOPPLER PRESSURE GRADIENTS MVA BY PHT CONTINUITY EQATION PISA MITRAL VALVE RESISTANCE PASP
MVA BY PLANIMETRY 2D Echo Best correlation with anatomical area Scanning method to avoid overestimation measured at leaflet tips in a plane perpendicular to mitral orifice Elliptical in shape Direct measure of mitral orifice including opened commissures in PSAX
Excessive gain setting may underestimate valve area Zoom mode is better for delineation Harmonic imaging can improve planimetry measurement Optimal time is mid diastole obtained by cine loop mode on a frozen image Multiple measurements in AF or incomplete commissural fusion difficult in calcified valve,chestdeformity and previous commissurotomy
Real time 3D echocardiography identify true smallest orifice independent of its orientation most accurate ultrasound technique for measuring MVA, with a superior pre- and postprocedural agreement with the Gorlin’s derived MVA Less experience dependent and more reproducible
Mitral leaflet separation (MLS) index Distance between the tips of the mitral leaflets in parasternal long-axis and four-chamber views it can be used as a semiquantitative method for the assessment of MS severity A value of 1.2 cm or more provided a good specificity and PPV for the diagnosis of non severe MS less than 0.8 cm -severe MS. It is not accurate in patients with heavy mitral valvular calcification and post BMV
PRESSURE GRADIENT Apical window CWD /PWD at or after tip of mitral valve Maximal and mean gradient Bernoulli equation( P =4V2) Derived from transmitral velocity flow curve Heart rate to be mentioned CD to identify eccentric mitral jet
Maximal gradient influenced by LA compliance and LV diastolic function In AF average of 5 cycles with least variation of R-R interval and as close possible to normal HR MVG dependent on HR,COP and associated MR Tachycardia, increased COP and associated MR overestimates gradient Maximal gradient is markedly affected
PRESSURE HALF TIME T1/2 is time interval in msecs between max mitral gradient in early diastole and time point where gradient is half max gradient Or it is the time when velocity falls to 1/1.414 peak PHT related to decceleration time PHT =.29x DT MVA=220/PHT
The empirically determined constant of 220 is proportional to the product of net compliance of left atrium and LV, and the square root of maximum transmitral gradient in a model that does not take into account active relaxation of LV
Obtained by tracing deceleration slope of E wave on Doppler spectral display Concave not feasible If slope is bimodal deceleration slope in mid diastole rather than early diastole is traced
Less dependent on COP or coexistent MR Useful when mean transmitral gradient is misleading MR -transmitral gradient overesimated Low COP –mean transmitral gradient -underestimated
Factors that may affect PHT by influencing LA pressure decline More rapid LA pressure decline shorten PHT LA draining to second chamber –ASD LA pressure drop rapidly PHT shortened Stiff LA –low LA compliance LA pressure drop rapidly PHT shortened
Factors affect PHT by influencing LV pressure rise More rapid LV pressure rise shorten PHT If LV fills from a second source PHT –AR LV pressure rise more rapidly PHT will be shortened If LV is stiff-low ventricular compliance LV pressure may rise more rapidly PHT will be shortened
All factors affect PHT (ASD, AR, low LA or LV compliance ) shorten PHT Leads to overestimation of MVA Therefore PHT never under estimate MVA Therefore if PHT >220 MS is severe If PHT is < 220 consider other methods to assess severity
Prosthetic MVA Not been validated Affected mainly by DD More accurate method is continuity equation
Not reliable After BMV Normally LA and LV compliance counteract each other when gradient and compliance are subject to important and abrupt changes alter relation between PHT and MVA Upto 48 hrs post BMV
CONTINUITY EQATION LVOT AREA
MVA X VTI mitral= LVOT area X VTI aortic MVA = LVOT area X VTI aortic VTI mitral MVA= pD2X VTI aortic 4 VTI mitral D is diameter of LVOT in CM and VTI in CM SV can be estimated from PA Method not useful in AF,AR or MR Useful in degenerative calcific MS