Download
1 / 12
120 likes | 366 Views
A Case of Secondary Hypogonadism. “Hypogonadism Due to Pituicytoma in an Identical Twin” H. H. Newnham & L. M. Rivera-Woll New Engl J Med 359 : 2824, 2008. W. Rose. Presentation and History

E N D
A Case of Secondary Hypogonadism “Hypogonadism Due to Pituicytoma in an Identical Twin” H. H. Newnham & L. M. Rivera-Woll New Engl J Med359: 2824, 2008 W. Rose
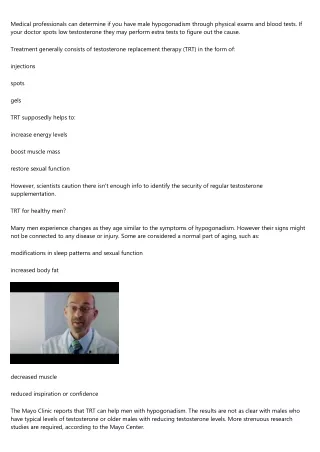
Presentation and History 43-year-old man (an identical twin) presents with 2-year history of lethargy, weakness, headaches; several-year history of gradual loss of body hair and declining libido. Left orchidopexy at 6 years of age. Physical Exam Shows features of hypopituitarism and hypogonadism, including central adiposity, nipple pallor, proximal muscle wasting, preservation of scalp hair, loss of body hair, gynecomastia, and right and left testicular volumes of 12 ml and 5 ml, respectively (normal volume, >15). Note contrast in appearance between hypogonadal patient (Panel A, right) and unaffected identical twin (left). Newnham, H.H. & L.M. Rivera-Woll (2008), New Engl J Med359: 2824.
Newnham, H.H. & L.M. Rivera-Woll (2008), New Engl J Med359: 2824.
Laboratory Tests Testosterone: 1.5 nmol per liter (normal range, 9.9 to 27.8). Follicle-stimulating hormone: 2.8 IU per liter (normal range, 1.5 to 12.4) Luteinizing hormone: 1.5 IU per liter (normal range, 1.7 to 8.6). Serum prolactin, thyroid function (measured by free thyroxine and thyroid-stimulating hormone), cortisol: normal. Insulin-like growth factor 1 level: mildly decreased. Newnham, H.H. & L.M. Rivera-Woll (2008), New Engl J Med359: 2824.
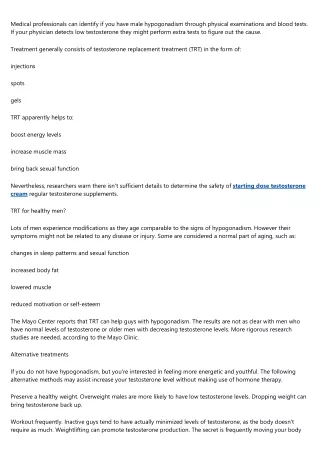
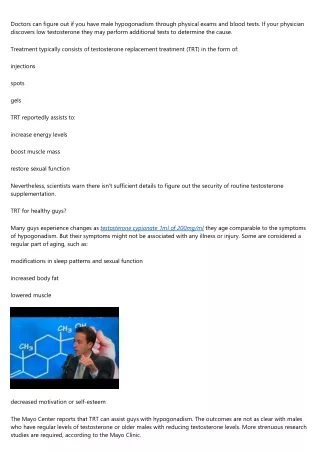
Imaging Magnetic resonance imaging of the pituitary showed a lobulated, contrast-enhancing suprasellar mass (16 by 29 mm; seen in the coronal view in Panel B [arrow] and in the sagittal view in Panel C [arrow]). Images of the unaffected twin are shown for comparison. Newnham, H.H. & L.M. Rivera-Woll (2008), New Engl J Med359: 2824.
Pituicytoma, MRI Normal, MRI Newnham, H.H. & L.M. Rivera-Woll (2008), New Engl J Med359: 2824.
Diagnosis Pituicytoma = pituitary cell tumor, confirmed by pathological analysis of tissue obtained from needle biopsy and subsequent surgery. Treatment Tumor excision by craniotomy. Followup Apart from a seizure, patient's postoperative recovery on pituitary-replacement therapy has been uneventful, with resolution of his symptoms. Newnham, H.H. & L.M. Rivera-Woll (2008), New Engl J Med359: 2824.
Comments Pituitary tumors usually grow slowly, don’t metastasize, and can be effectively treated by surgical removal. Pituitary tumors can be secretory or non-secretory. A secretory tumor makes one or more of the hormones made by a normal pituitary, but makes the hormones in an uncontrolled way (i.e. too much). W. Rose
Discussion Questions Why are testes small and testosterone low? Why is L testis smaller than R? What do FSH & LH do, and where are they produced? In a male with a normal pituitary, how would FSH and LH levels respond to low testosterone? Compare to this patient. Why are levels of prolactin, thyroid hormone and TSH, cortisol, and IGF-1 checked and reported? (Which are made in pituitary, which are regulated by pituitary?) Is this pituitary tumor secretory or non-secretory? Why do you say so? Suprasellar? W. Rose
Discussion Questions What symptom might be expected that was not seen? How would you do a needle biopsy or remove the tumor? What structures would you be especially careful to avoid? If anterior pituitary (adenohypophysis) were completely removed, what hormones would have to be monitored and replaced exogenously? If posterior pituitary (neurohypophysis) were also removed, what hormones would be added to the list? W. Rose
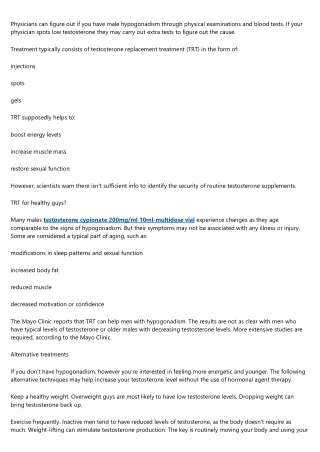
Conventional transphenoidal approach. Coronal section Craniotomy and subfrontal approach. Tew, JM, Jr, van Loveren, HR, Keller, JT; Atlas of Operative Microneurosurgery, Volume II; W.B. Saunders, 2002, retreived on 2009-01-08 from http://www.mayfieldclinic.com/PE-surgpit.htm. W. Rose
Endoscopic transphenoidal approach http://www.ent.uci.edu/endoscopic_pituitary_tumor.htm Animation of different surgical approaches to pituitary tumors available at http://www.skullbaseinstitute.com/animations.htm W. Rose