Download
1 / 1
10 likes | 155 Views
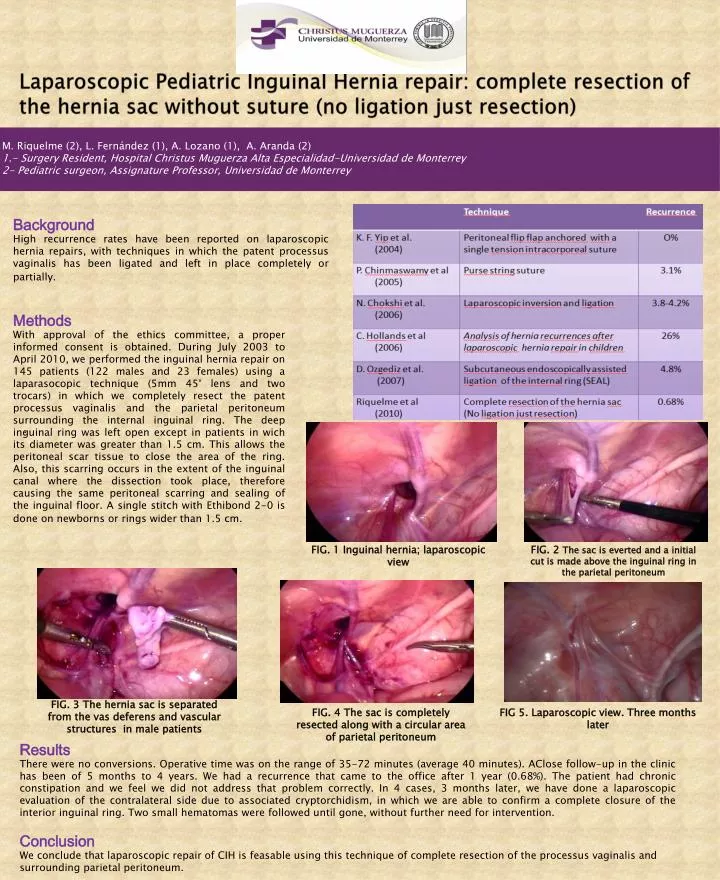
Laparoscopic Pediatric Inguinal Hernia repair: complete resection of the hernia sac without suture (no ligation just resection). M . Riquelme (2), L. Fernández (1), A. Lozano (1), A. Aranda (2) 1.- Surgery Resident , Hospital Christus Muguerza Alta Especialidad-Universidad de Monterrey

E N D
Laparoscopic Pediatric Inguinal Hernia repair: complete resection of the hernia sac without suture (no ligation just resection) M. Riquelme (2), L. Fernández (1), A. Lozano (1), A. Aranda (2) 1.- SurgeryResident, Hospital Christus Muguerza Alta Especialidad-Universidad de Monterrey 2- Pediatricsurgeon, AssignatureProfessor, Universidad de Monterrey Background High recurrence rates have been reported on laparoscopic hernia repairs, with techniques in which the patent processusvaginalis has been ligated and left in place completely or partially. Methods With approval of the ethics committee, a proper informed consent is obtained. During July 2003 to April 2010, we performed the inguinal hernia repair on 145 patients (122 males and 23 females) using a laparasocopic technique (5mm 45° lens and two trocars) in which we completely resect the patent processusvaginalis and the parietal peritoneum surrounding the internal inguinal ring. The deep inguinal ring was left open except in patients in wich its diameter was greater than 1.5 cm. This allows the peritoneal scar tissue to close the area of the ring. Also, this scarring occurs in the extent of the inguinal canal where the dissection took place, therefore causing the same peritoneal scarring and sealing of the inguinal floor. A single stitch with Ethibond 2-0 is done on newborns or rings wider than 1.5 cm. • . FIG. 1 Inguinal hernia; laparoscopicview FIG. 2 The sac is everted and a initial cut is made above the inguinal ring in the parietal peritoneum FIG. 3 The hernia sac is separated from the vas deferens and vascular structures in male patients FIG. 4 The sac is completely resected along with a circular area of parietal peritoneum FIG 5. Laparoscopic view. Three months later Results There were no conversions. Operative time was on the range of 35-72 minutes (average 40 minutes). AClosefollow-up in the clinic has been of 5 months to 4 years. We had a recurrence that came to the office after 1 year (0.68%). The patient had chronic constipation and we feel we did not address that problem correctly. In 4 cases, 3 months later, we have done a laparoscopic evaluation of the contralateral side due to associated cryptorchidism, in which we are able to confirm a complete closure of the interior inguinal ring. Two small hematomas were followed until gone, without further need for intervention. Conclusion We conclude that laparoscopic repair of CIH is feasable using this technique of complete resection of the processusvaginalis and surrounding parietal peritoneum.