Download
1 / 86
970 likes | 1.39k Views
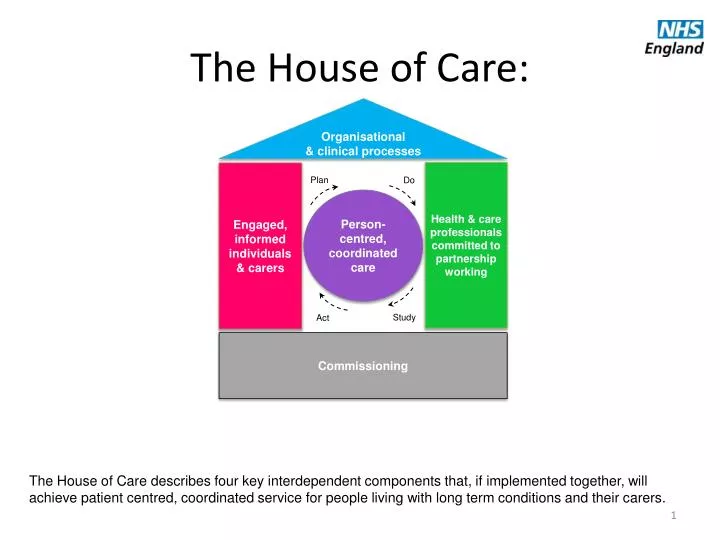
The House of Care:. Organisational & clinical processes. Health & care professionals committed to partnership working. Engaged, informed individuals & carers. Plan. Do. Person-centred, coordinated care. Study. Act. Commissioning.

E N D
The House of Care: Organisational & clinical processes Health & care professionals committed to partnership working Engaged, informed individuals & carers Plan Do Person-centred, coordinated care Study Act Commissioning The House of Care describes four key interdependent components that, if implemented together, will achieve patient centred, coordinated service for people living with long term conditions and their carers.
Building the House – The House of Care Toolkit • Aframework to bring together all the relevant national guidance, published evidence, local case studies and information for patients and their carers. • It includes information on what tools and resources are required to achieve person-centred coordinated care and how these can be effectively commissioned. • Resources are arranged into the four key components of the House with summaries of the impact that could be achieved, based on current evidence and details about where to find additional information.
To Enter the House first chose your level: Local National Personal Supporting for professionals, services users and carers to work together to understand, plan and deliver person centred coordinated care. National and international guidance, evidence, tools and resources that will enable the construction of the House of Care at the next two levels. Examples of local examples of good practice that will inform the commissioning of services at a local level .
Click on the links below for more information about each component and use this to build your own house Organisational and Clinical Processes Build my own house • Guidelines, evidence and national audits • Care Delivery • Information and technology • Care Planning • Safety and Experience Person centred- coordinated care Informed and engaged patients and carers Health and Care Professionals committed to partnership working • Self management • Information and Technology • Group and peer support • Care Planning • Carers • Integration • Culture • Workforce • Technology • Care Co-ordination • Care Planning Commissioning • Service User and Public Involvement • Contracting and procurement • Needs Assessment and Planning • Joint commissioning of services • Metricsand Evaluation • Care Planning • Tools and levers
Person centred- coordinated care Enables individuals to make informed decisions which are right for them, and empower them to self-care for their long term conditions in partnership with health and care professionals. It relies on four key components, all of which must be present for the goal, person-centred coordinated care, to be realised • Commissioning– which is not simply procurement but a system improvement process, the outcomes of each cycle informing the next one. • Engaged, informed individuals and carers – enabling individuals to self-manage and know how to access the services they need when and where they need them. • Organisational and clinical processes– structured around the needs of patients and carers using the best evidence available, co-designed with service users where possible. • Health and care professionals working in partnership– listening, supporting, and collaborating for continuity of care. Back to house
Integration Ensuring care is designed and delivered around the needs of the individual. Integration is particularly important for people with complex care needs. Services should be joined-up to promote improved outcomes for individuals in need of health and social support, enabling them to live not just longer, but better lives. Care is planned with people who work together to understand me and my carer(s), put me in control, co-ordinate and deliver services to achieve my best outcomes Health & care professionals committed to partnership working Back to house • Interdisciplinary working • Professionals from different organisations across health and social care and the voluntary sector working closely together ensuring that care feels coordinated to people living with long term conditions and their carers. • Key Components • Single point of contact • Multi disciplinary team working • Professionals talk to each other • Services quick and responsive people are promoted to stay independent and active • Care developed around the individual and not the system • Care Transition • Ensuring a seamless transition for people with long term conditions between different care settings. • Key Components • Transition following discharge from hospital • Transition related to changes in long term care needs • Transition from children's to adult services.
Interdisciplinary Working Health & care professionals committed to partnership working Resources Integrated care for patients and populations: Improving outcomes by working together - A report to the Department of Health and the NHS Future Forum, The Kings Fund http://www.kingsfund.org.uk/publications/integrated-care-patients-and-populations-improving-outcomes-working-together Integrated Care and Support Pioneers programme, NHS IQ http://www.nhsiq.nhs.uk/improvement-programmes/long-term-conditions/integrated-care.aspx Integrated Care – Better Care Fund – Local Government Association http://www.local.gov.uk/web/guest/health-wellbeing-and-adult-social-care/-/journal_content/56/10180/4096799/ARTICLE Integrated care value case toolkit http://www.local.gov.uk/health-wellbeing-and-adult-social-care/-/journal_content/56/10180/4060433/ARTICLE ICASE - Integrated Care Support and Exchange http://www.icase.org.uk/pg/dashboard Kings Fund Integrated care: making it happen http://www.kingsfund.org.uk/projects/integrated-care-making-it-happen Back to integration
Care Transition Health & care professionals committed to partnership working Resources Lost in transition, Moving young people between child and adult health services, Royal College of Nursing http://www.rcn.org.uk/__data/assets/pdf_file/0010/157879/003227_WEB.pdf Transitions between children’s and adult’s health services, and the role of voluntary and community children’s sector, VSS POLICY BREIFING http://www.ncb.org.uk/media/42225/transition_to_adult_services_vss_briefing.pdf Transition, National Council for Palliative Care http://www.ncpc.org.uk/transitions Coordinated transition between health and social care, NICE http://www.nice.org.uk/media/7C5/66/TranstionBetweenHealthAndSocialCareDraftScope.pdf Back to integration
Culture To promote an environment where people with long term conditions, their carers and professionals involved in their care have an equal relationship and a joint responsibility for managing their care. To ensure parity of esteem where physical health is valued equally with mental health. Health & care professionals committed to partnership working Back to house • Promoting a partnership approach to care • To better involve patients in decisions about their own health • to facilitate self-care. • Key Components • Developing equal relationships between patients and professionals • Sharing information to support patients to self-care • Parity of Esteem • People with poor physical health are at higher risk of experiencing mental health problems and people with poor mental health are more likely to have poor physical health. • Key Components • Valuing mental health and physical health equally. • Considering the physical impact of living with a mental health condition and the mental health impact of living with a long term condition • Clinical Champions and Professional Support • Effective leadership from professional bodies us key to embedding the type of culture change that is needed. • Key Components • Supporting the workforce to adjust to a new way of working • Governance • Professional practice • Cultural relationships.
Promoting a partnership approach to care Resources Shared decision making, NHS England http://www.england.nhs.uk/ourwork/pe/sdm/ Measuring Shared Decision Making A review of research evidence, NHS Right Care http://www.rightcare.nhs.uk/wp-content/uploads/2012/12/Measuring_Shared_Decision_Making_Dec12.pdf Changing the culture: resources developed by AQuA, NHS England http://www.england.nhs.uk/ourwork/pe/sdm/resources/aqua/ Health & care professionals committed to partnership working Back to culture
Clinical champions and professional support Health & care professionals committed to partnership working Resources Care Planning, Royal College of General Practitioners http://www.rcgp.org.uk/clinical-and-research/clinical-resources/care-planning.aspx 6 C’s Compassion in Practice, NHS England http://www.england.nhs.uk/nursingvision/ Association for Directors of Adult Social Services http://www.adass.org.uk/ Royal College of Nursing https://www.rcn.org.uk/ Back to culture
Parity of Esteem Health & care professionals committed to partnership working Resources Valuing mental health equally with physical health or “Parity of Esteem”, NHS England http://www.england.nhs.uk/ourwork/qual-clin-lead/pe/ Long-term conditions and mental health The cost of co-morbidities, The Kings Fund http://www.kingsfund.org.uk/publications/long-term-conditions-and-mental-health?gclid=CPCbxbyoxrwCFeXKtAodh0YA4g Mental Health Partnerships http://mentalhealthpartnerships.com/ Back to culture
Workforce Ensuring that the workforce is configured to support partnership working both between different professional groups and between services users and professionals providing care. This will include considerations regarding integration of the workforce to provide a coordinated approach to people living with long term conditions and clarification of roles and responsibilities of professionals and opportunities for training. Health & care professionals committed to partnership working Back to house • Integration • The long term conditions workforce should offer a seamless pathway of care to patients and carers. Effective workforce integration should be in place to achieve this. • Key Components • Joint training • Skill mix • Joint health and social care roles • Communication • Multi-disciplinary team working • Roles, responsibilities and training • Ensuring the workforce supporting people living with long term conditions are aware of the role they play and are appropriately trained. • Key Components • Continuing professional development • Person specifications • Training
Integration Resources Integrated care for patients and populations: Improving outcomes by working together - A report to the Department of Health and the NHS Future Forum, The Kings Fund http://www.kingsfund.org.uk/publications/integrated-care-patients-and-populations-improving-outcomes-working-together Integrated Care – Better Care Fund – Local Government Association http://www.local.gov.uk/web/guest/health-wellbeing-and-adult-social-care/-/journal_content/56/10180/4096799/ARTICLE Coordinated transition between health and social care, NICE http://www.nice.org.uk/media/7C5/66/TranstionBetweenHealthAndSocialCareDraftScope.pdf Integrated Care and Support: Our Shared Commitment https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/198748/DEFINITIVE_FINAL_VERSION_Integrated_Care_and_Support_-_Our_Shared_Commitment_2013-05-13.pdf Health & care professionals committed to partnership working Back to workforce
Roles, responsibilities and training Resources Long Term Conditions, Skills for Health http://www.skillsforhealth.org.uk/service-area/long-term-conditions/ Delivering better services for people with long-term conditions Building the house of care, Kings Fund http://www.kingsfund.org.uk/sites/files/kf/field/field_publication_file/delivering-better-services-for-people-with-long-term-conditions.pdf Health & care professionals committed to partnership working Back to workforce
Information and Technology Information systems and technology that facilitate equal relationships between people with long term conditions, their carers and professionals providing their care. This may be achieved through better access to information or technology to allow patients to have a greater role in condition management. Health & care professionals committed to partnership working Back to house • Shared information systems • Facilitating the sharing of information between different professional groups involved in the care of an individual to improve the management of care. • Sharing information will aim to ensure the wider need for the individual are considered by all professionals involved in their care. • Key Components • Joint care plans • Shared access or joint information systems across health organisations and between health and social care • Patient Held Record • The patient is given a copy of the record to keep, and to take to health appointments, to help manage healthcare tasks and communication. • PHRs are formal and structured records that are given to patients to enable the continuity and quality of care. • Key Components • Structured sections of patient and healthcare information • Blank sections to enable patient note-taking and healthcare staff notes
Shared Information Systems Resources Technical Approaches for Sharing Care Plans, NHS QIPP Workstream http://www.connectingforhealth.nhs.uk/systemsandservices/qipp/library/careplans.pdf Summary Care Record, Health and Social Care Information Centre http://systems.hscic.gov.uk/scr Health & care professionals committed to partnership working Back to information and technology
Patient Held Record Resources Summary Care Records, NHS Choices http://www.nhs.uk/NHSEngland/thenhs/records/healthrecords/Pages/servicedescription.aspx Enabling patients to access electronic health records Guidance for health professionals, Royal College of General Practitioners http://www.rcgp.org.uk/clinical-and-research/practice-management-resources/health-informatics-group/~/media/Files/CIRC/Health%20Informatics%20Report.ashx Patient record access: turning it on, sharing the learning, The Health Foundation http://www.health.org.uk/areas-of-work/programmes/closing-the-gap-through-changing-relationships/related-projects/patient-record-access/ Health & care professionals committed to partnership working Back to information and technology
Co-ordination of care Supporting people to better understand the health and social care system so that they can get the support they require when they need it. This can range from a person having a named professional as a first point of contact with the health system to a case manager responsible for coordinating the health and social care for people with multiple complex long term conditions. Health & care professionals committed to partnership working Back to house • Case Management • A targeted, community-based and pro-active approach to care that • involves case-finding, assessment, care planning, and care co-ordination • accurate case-finding to ensure patients with highly complex and multiple conditions receive high-intensity professional support. • Key Components: • Processes to identify those suitable for case management are in place • Case managers have an appropriate case load • Case managers are able to effectively coordinate car e • Care Co-ordination • Supporting individuals find their way around the, sometimes complex services provided by health and social care. • Key Components • Care navigators • Directory of services • Identifying and assessing needs for people living with long term conditions and their carers • Ability to identify the most appropriate services for the individual • Developing support plans
Case Management Resources Case Management, What it is and how it can best be implemented, The Kings Fund http://www.kingsfund.org.uk/sites/files/kf/Case-Management-paper-The-Kings-Fund-Paper-November-2011_0.pdf Case management and community matrons for long term conditions, British Medical Journal http://www.bmj.com/content/329/7477/1251 Health & care professionals committed to partnership working Back to co-ordination of care
Care Co-ordination Resources Safer passage: how care navigators help improve mental health services, Health Services Journal http://www.hsj.co.uk/resource-centre/best-practice/local-integration-resources/safer-passage-how-care-navigators-help-improve-mental-health-services/5041420.article# Co-ordinated care for people with complex chronic conditions, Kings Fund http://www.kingsfund.org.uk/projects/co-ordinated-care-people-complex-chronic-conditions Care co-ordination through integrated health and social care teams, Kings Fund http://www.kingsfund.org.uk/projects/gp-commissioning/ten-priorities-for-commissioners/care-coordination Health & care professionals committed to partnership working Back to co-ordination of care
Care Planning Professionals need to recognise that the personal assets that patients (and their families) bring to the care planning process are as important as the clinical information in the medical record. They must ensure contacts people with long term conditions, their carers and have meet their physical, social and emotional wellbeing needs and best support them to manage their condition. Effective care planning requires both patients and professionals to adequately prepared in advance and are clear about the purpose of the care planning process. Health & care professionals committed to partnership working Back to house • Care Planning • An interactive partnership between clinician and patient supporting self management . • Key Components • Information should be given to the patient prior to the appointment • During the appointment achievable goals should be set in partnership. • Ongoing process • Capturing gaps between preferences and care received and feeding back these preferences to inform future planning. Motivational support • Facilitating healthy, sustainable behaviour change by supporting people living with long term conditions to take a more active role in their own care. To do this, people require skilled support and motivation from their clinicians. • Key Components • Motivational interviewing techniques • Health coaching • Usinga guiding style to engage with patients • Clarify strengths and aspirations, evoke their own motivations for change, and promote autonomy of decision making.
Care planning Resources Shared decision making, NHS England http://www.england.nhs.uk/ourwork/pe/sdm/ Tools for shared decision making, NHS England http://www.england.nhs.uk/ourwork/pe/sdm/tools-sdm/ Care Planning, Royal College of General Practitioners http://www.rcgp.org.uk/clinical-and-research/clinical-resources/care-planning.aspx Embedding SDM in NHS care: Resources developed by Capita, NHS England http://www.england.nhs.uk/ourwork/pe/sdm/resources/capita/ Health & care professionals committed to partnership working Back to care planning
Motivational Support Health & care professionals committed to partnership working Resources Motivational Interviewing in Primary Care, Tim Anstiss http://www.networks.nhs.uk/discussion/soapbox/130950854/232769575/motivational-interviewing-in-primary-care-pdf Motivational interviewing 1: background, principles and application in healthcare, The Nursing Times http://www.nursingtimes.net/motivational-interviewing-1-background-principles-and-application-in-healthcare/5018759.article Health Coaching, NHS Direct http://www.nhsdirect.nhs.uk/Commissioners2/HealthCoaching Co-creating Health, Health Foundation http://www.health.org.uk/areas-of-work/programmes/co-creating-health/ Back to care planning
Organisational and Clinical Processes Care Planning The organisation of health and social care services practices should be structured to support the care planning process. The process involves professionals working in partnership with people living with long term conditions and their carers, identifying priorities, discussing care and support options, agreeing goals they can achieve themselves, and co-producing a single care plan, that meets their physical, social and emotional wellbeing needs regardless of how many long-term conditions they have. Back to house • Recording Outputs of Care Planning Consultations • Processes are in place that allow information captured in care planning appointments to be recorded to inform future care planning consultations and future service provision. • Key Components • Information systems to records agreed goals • Access to menus of available services to support individuals to achieve their goals • Information systems to record gaps between individual preferences and services provided to inform commissioning • Care Planning Structure • Services should to be configured to support the ongoing collaborative care planning process. • Key Components • Allowing time for multiple long term conditions to be considered where required • Allowing information on clinical test results to be provided to the patient and the professional prior to the care planning discussion • Considering the frequency of appointments and reviews to provide an opportunities to review short and longer term goals and have mechanisms in place for patient recall
Organisational and Clinical Processes Care Planning Structure Resources Partners in Care: A Guide to Implementing a Care Planning Approach to Diabetes Care, NHS Diabetes https://www.diabetes.org.uk/Documents/nhs-diabetes/care-planning/partners-in-care-implementing-care-planning-approach.pdf Care Planning Improving the Lives of People with Long Term Conditions, Royal College of General Practitioners http://www.rcgp.org.uk/clinical-and-research/clinical-resources/~/media/Files/CIRC/Cancer/Improving%20the%20Lives%20of%20people%20with%20LTC%20-%202012%2005%2009.ashx Back to care planning
Organisational and Clinical Processes Resources Partners in Care: A Guide to Implementing a Care Planning Approach to Diabetes Care, NHS Diabetes https://www.diabetes.org.uk/Documents/nhs-diabetes/care-planning/partners-in-care-implementing-care-planning-approach.pdf Back to care planning
Organisational and Clinical Processes Safety and Experience People with long term conditions should receive high quality care that is safe and reliable and that also delivers excellent patient experience. Processes should be in place to ensure patient experience is captured and to allow safety concerns to be identified and risks for future incidents to be reduced. Back to house • Experience • Ensuring processes are in place so that the experience of the service users can be recorded and reviewed so that services delivered reflect the needs and preferences of people living with long term conditions and their carers. • Key components • Mechanisms are in place to capture the experiences of people living with long term conditions and their families and carers • These experiences inform future planning and delivery of services • Safety • Promoting an active safety management approach to identify potential risk while helping to improve monitoring and measuring of safety indicators. • Key Components • Evidence based procedures in place promoting safety • Potential safety concerns identified and addressed • Processes for identifying adverse incidents and near misses • Safety concerns are freely raised and openly discussed • Safe processes to optimise the use of medicines
Organisational and Clinical Processes Safety Resources Patient Safety, NHS England http://www.england.nhs.uk/ourwork/patientsafety/ European Union Network for Patient Safety and Quality of Care http://www.pasq.eu/ Patient Safety Resource Centre, The Health Foundation http://patientsafety.health.org.uk/?gclid=COHtiuyQ07wCFSgKwwodbj0Axg Patient Safety, Practical information, tools and support to improve patient safety in the NHS http://www.nrls.npsa.nhs.uk/ Medicines Optimisation: Helping patients to make the most of medicines Good practice guidance for healthcare professionals in England, Royal Pharmaceutical Society. http://www.rpharms.com/promoting-pharmacy-pdfs/helping-patients-make-the-most-of-their-medicines.pdf Good practice in prescribing and managing medicines and devices, General Medical Council http://www.gmc-uk.org/Prescribing_Guidance__2013__50955425.pdf Back to safety and experience
Organisational and Clinical Processes Experience Resources Improving Patient Experience, NHS England http://www.england.nhs.uk/ourwork/pe/ 6 C’s Compassion in Practice, NHS England http://www.england.nhs.uk/nursingvision/ Transforming Patient Experience, NHS Institute http://www.institute.nhs.uk/patient_experience/guide/the_patient_experience_research.html Patient Experience, Kings Fund http://www.kingsfund.org.uk/topics/patient-experience Back to safety and experience
Organisational and Clinical Processes Information and Technology Information and technology is a key factor underpinning successful organisational and clinical processes to support people living with long term conditions and their carers. Two Important elements of this are how information and technology can be used to identify which Individuals in a population will most benefit from care and to share information about these individuals both within and between organisations. Back to house • Information systems • Professionals are required to have timely and relevant access to information in order to effectively manage people living with long term conditions. • Key Components • Information sharing and access of records across organisational boundaries • Integrated information systems is key to ensuring the care is delivered around the needs of the individual as a whole. • Risk Stratification • Using relationships in historic population data to estimate the future use of health care services for each member of a population. • Key Components • Use of information from primary and secondary care services in addition to social care data • Useful both for population planning purposes and for identifying which patients should be offered targeted, preventive support.
Organisational and Clinical Processes Risk Stratification Resources Risk Stratification, NHS England http://www.england.nhs.uk/ourwork/tsd/ig/risk-stratification/ Predicting and reducing re-admission to hospital, The Kings Fund http://www.kingsfund.org.uk/projects/predicting-and-reducing-re-admission-hospital RISKPROFILING AND CARE MANAGEMENT SCHEME, NHS England http://www.england.nhs.uk/wp-content/uploads/2013/03/ess-risk-profiling.pdf Risk Prediction Network, NHS networks http://www.networks.nhs.uk/nhs-networks/risk-prediction-network/?searchterm=risk%20stratification Information Governance and Risk Stratification: Advice and Options for CCGs and GPs http://www.england.nhs.uk/wp-content/uploads/2013/06/ig-risk-ccg-gp.pdf Advice on Risk Prediction and Stratification, London: National Information Governance Board for Health and Social Care, July 2012 http://www.nigb.nhs.uk/pubs/guidance/riskpred.pdf Back to information and technology
Organisational and Clinical Processes Information Systems Resources Better information means better care, NHS England http://www.england.nhs.uk/ourwork/tsd/care-data/ Keeping your online health and social care records safe and secure, NHS England http://www.nhs.uk/NHSEngland/thenhs/records/healthrecords/Documents/ PatientGuidanceBooklet.pdf New technology can improve the health services delivered to millions of people, NHS England http://www.england.nhs.uk/2013/11/15/new-tech-imprv-hlt-serv/ Back to information and technology
Organisational and Clinical Processes Guidelines, Evidence and National Audits Ensuring the services delivered to provide person centred care for people living with long term conditions follow the appropriate guidelines and based on robust evidence where this is available. Back to house • Evidence Based Practice • The use of robust evidence to inform the commissioning and delivery of services in practice. • Where evidence is not available this may involve working with academic institutions to contribute to the body of evidence available. • Key Components • Routine use of evidence in service planning and delivery • Guidelines • To help professionals deliver the best possible care offering the best value for money. • Key Components • Independent, authoritative and evidence-based information • Effective ways to prevent, diagnose and treat disease and ill health, reducing inequalities and variation. • Specific diseases as well as generic principles for care. • National Audits • Audits allow health organisations to compare their performance against specific standards and national trends, enabling them to deliver better care for their patients. • Key Components • Usually conducted in disease specific areas such as COPD, Kidney Diseaseor Stroke.
Organisational and Clinical Processes Guidelines Resources National Institute of Clinical Excellence http://www.nice.org.uk/ Social Care Institute for Excellence http://www.scie.org.uk/ Map of Medicine http://www.mapofmedicine.com/ End of Life Care Quality Standard, Public Health England http://www.endoflifecare-intelligence.org.uk/national_information_standard/ British National Formulary http://www.bnf.org/bnf/index.htm Back to guidelines and national audits
Organisational and Clinical Processes National Audits Resources Clinical audits, Health and Social Care Information Centre http://www.hscic.gov.uk/clinicalaudits Audit and Quality Improvement, British Thoracic Society https://www.brit-thoracic.org.uk/audit-and-quality-improvement/ Audits, University College London http://www.ucl.ac.uk/nicor/audits GRASP Audit Tools, PRIMIS http://www.nottingham.ac.uk/primis/index.aspx Back to guidelines and national audits
Organisational and Clinical Processes Evidence Based Practice Resources NICE Evidence Search Health and Social Care, NICE http://www.evidence.nhs.uk/ The Cochrane Library http://www.thecochranelibrary.com/ Social Care Institute for Excellence http://www.scie.org.uk/ Shared Learning Implementing Evidence Based Practice, NICE http://www.nice.org.uk/usingguidance/sharedlearningimplementingniceguidance/shared_learning_implementing_nice_guidance.jsp Back to guidelines and national audits
Organisational and Clinical Processes Care Delivery How services and processes are configured to up to promote a person centred approach to care as people with long term conditions move through the health and social care system. This will include how to ensure care is being provided in the most clinically appropriate place whilst paying regard to quality of life and efficiency. Back to house • Care Closer to Home • Ensuring processes are in place to allow people living with long term conditions to be cared for in a community setting where this is clinically appropriate. • Key Components • Access to specialist clinics in the community • Pathways to prevent admission and to facilitate earlier discharge from hospital. • Workforce • Ensuring workforce processes support professionals to deliver person centred co-ordinated care for people living with long term conditions. • Key Components • Training of medical, nursing allied health professionals and social care workforce • Consideration of the skill mix of the workforce • Rehabilitation • Following condition exacerbations rehabilitation may be required to promote recovery and prevent further exacerbations. • Key Components • Generic rehabilitation programmes such as social care support to return home safely • Condition specific e.g. stroke or pulmonary rehabilitation.
Organisational and Clinical Processes Workforce Resources Long Term Conditions, Skills for Health http://www.skillsforhealth.org.uk/service-area/long-term-conditions/ Improving services for people with long-term conditions through large-scale workforce change, NHS Employers http://www.nhsemployers.org/SiteCollectionDocuments/Improving_services_for_people_with_long-term_conditions_through_large_scale_workforce_change_sc_140906.pdf Long term conditions e-learning tools for NHS and social care workforce, Department of Health https://www.gov.uk/government/news/long-term-conditions-e-learning-tools-for-nhs-and-social-care-workforce Back to care delivery
Organisational and Clinical Processes Care closer to home Resources Avoiding hospital admissions Lessons from evidence and experience, The Kings Fund http://www.kingsfund.org.uk/sites/files/kf/field/field_publication_file/avoiding-hospital-admissions-lessons-from-evidence-experience-ham-imison-jennings-oct10.pdf Interventions to reduce unplanned hospital admissions: a series of systematic reviews, Purdy S. et al (June 2012) http://www.bristol.ac.uk/primaryhealthcare/docs/projects/unplannedadmissions.pdf Avoiding hospital admissions What does the research say? The Kings Fund http://www.kingsfund.org.uk/sites/files/kf/Avoiding-Hospital-Admissions-Sarah-Purdy-December2010_0.pdf Back to care delivery
Organisational and Clinical Processes Rehabilitation Resources Pulmonary Rehabilitation, National Institute of Clinical Excellence http://www.nice.org.uk/guidance/qualitystandards/chronicobstructivepulmonarydisease/pulmonaryrehabilitation.jsp Stroke Rehabilitation, National Institute of Clinical Excellence http://guidance.nice.org.uk/CG162 Improving Patient Outcomes through restructuring Recovery, Rehabilitation and Re-ablement, Department of Health http://www.nhsconfed.org/Training/Documents/RRR%20redesign.pdf Back to care delivery
Engaged, informed individuals and carers Self management Empowering people with the confidence and information to look after themselves when they can, and visit the GP when they need to, giving people greater control of their own health and encourages healthy behaviours that help prevent ill health in the long-term. Back to house • Personal budgets • Personal health budgets are money in lieu of NHS and social care services. They can be spent on a range of care and support, including things which are not traditionally commissioned. They are a tool for commissioning services at the level of the individual. • Key Components • Assessment of goals for the personal health budget • Agreed care plan between the NHS and the individual • Lifestyle • Promoting healthy lifestyle choices for people living with long term conditions to ensure they experience a good quality of life and to reduce their likelihood of developing further conditions and to reduce their impact on health and social care service. • Key Components • Every contact counts • Targeted smoking cessation services • Weight management services • Exercise programmes • Activation • Activation is a measure of an individual’s knowledge, • skill, and confidence for self-management. Higher levels of activation have been associated with reduced healthcare utilisation and positive changes in self management behaviour. • Key Components • Assessment of the activation levels • Tailoring support levels of activation • Mechanisms to increase activation levels
Engaged, informed individuals and carers Personal Budgets Resources Personal health budgets, NHS England http://www.personalhealthbudgets.england.nhs.uk Building on a people’s movement for change, People Hub www.peoplehub.org.uk Personal Health Budgets Evaluation https://www.phbe.org.uk/ Personal Health Budgets Toolkit, NHS England http://www.personalhealthbudgets.england.nhs.uk/Topics/Toolkit/index.cfm Direct payments and personal budgets for social care - Commons Library Standard Note http://www.parliament.uk/business/publications/research/briefing-papers/SN03735/direct-payments-and-personal-budgets-for-social-care Back to self management
Engaged, informed individuals and carers Lifestyle Resources Making Every Contact Count, NHS Yorkshire and Humber http://www.makingeverycontactcount.co.uk/ The NHS’ role in the public’s health, NHS Future Forum https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/216423/dh_132114.pdf Enabling People to Live Well, The Health Foundation http://www.health.org.uk/publications/enabling-people-to-live-well/ Self Care Forum http://www.selfcareforum.org/ Back to self management
Engaged, informed individuals and carers Activation Resources Changing the culture: resources developed by AQuA, NHS England http://www.england.nhs.uk/ourwork/pe/sdm/resources/aqua/ Summary of the Evidence on Performance of the Patient Activation Measure (PAM), NHS Kidney Care http://selfmanagementsupport.health.org.uk/media_manager/public/179/SMS_resource-centre_publications/PatientActivation-1.pdf Back to self management
Engaged, informed individuals and carers Information and Technology Information and technology is a key factor to supporting people living with long term conditions and their carers to feel engaged with and informed about their care. Professionals should ensure information provided is tailored to meet the needs of the individual. Technology such has telehealth or mobile apps can be used to give individuals independence and allow them to play a greater role in managing their care. Technology can also be used to give people alternative ways of accessing information, education and services. Back to house • Information • Personalised packages of information designed to help people with long-term conditions to feel more informed and more in control of their health and wellbeing. • Key Components • Information on conditions, treatments, services and support available. • Provision of a personalised information resource based on an assessment of the individual’s information needs. • Digital health • In addition to telehealth and telecare there are other forms of technology that can support people living with long term conditions and there carers. • Key Components • Mobile apps • Video or internet based consultations • Online forums • Social networking • Email and text contacts • Online education resources • Telehealth and telecare • Telecare and telehealth services use technology to help people live more independently at home. They include personal alarms and health-monitoring devices • Key Components • Assessment of who will benefit most from telehealth/telecare • Joint assessment and referral process • Service structures to underpin telehealth and telecare
Engaged, informed individuals and carers Digital Health Resources NHS Choices Health Apps Library, NHS Choices http://apps.nhs.uk/ Long Term Condition Management, Airedale Digital Healthcare Centre http://www.airedaledigitalhealthcarecentre.nhs.uk/Long_Term_Condition_Management/ Back to technology
Engaged, informed individuals and carers Telehealth and Telecare Resources Telecare and telehealth technology, NHS Choices http://www.nhs.uk/Planners/Yourhealth/Pages/Telecare.aspx Telehealth and telecare, The Kings Fund http://www.kingsfund.org.uk/topics/telecare-and-telehealth 3 million lives http://3millionlives.innovation.nhs.uk/pg/dashboard The impact of telehealth and telecare: the Whole System Demonstrator project, Nuffield Trust http://www.nuffieldtrust.org.uk/our-work/projects/impact-telehealth-and-telecare-evaluation-whole-system-demonstrator-project Back to technology
Engaged, informed individuals and carers Information Resources Information Prescription Service, NHS Choices http://www.nhs.uk/ipg/Pages/IPStart.aspx NHS Choices http://www.nhs.uk/Pages/HomePage.aspx Information prescriptions - an e learning tool, NHS Employers http://www.nhsemployers.org/PlanningYourWorkforce/educationandtraining/LongTermConditions/InformationPrescriptions/Pages/AboutInformationPrescriptions_Final.aspx Getting the most out of information prescriptions, Macmillan http://www.macmillan.org.uk/Documents/Newsletter/InfoPrescriptionsBooklet2012.pdf Social prescribing for mental health – a guide to commissioning and delivery, Care Services Improvement Partnership – North West http://www.centreforwelfarereform.org/uploads/attachment/339/social-prescribing-for-mental-health.pdf Back to technology
Group and Peer support Patients, carers and volunteer members of the public can offer opportunities to support people living with long term conditions. This support can be offered in the community, through groups set up specifically for this purpose or on an individual level. Peer support is often effective as the people providing the support often have first hand experience of living with a long term condition or caring for someone who does. In addition to the educational impact of courses, many patients value the social support gained from meeting other people who are living with a long-term condition Engaged, informed individuals and carers Back to house • Peer support groups • Peer-led support groups are proven to help people manage long-term conditions by reducing depression, building self-esteem and improving physical and mental health. • Key Components • Awareness of peer-support programmes that are available • Peer-support groups are considered in the care planning process • Community health champions • People who, with training and support, voluntarily bring their ability to relate to people and their own life experience to transform health and well-being in their communities • Key Components • Champions become involved in community groups/events and offer informal support people to join in healthy activities • Lay educator programmes • A Lay Educator is someone who delivers group education to people with a long term condition alongside a professional. A Lay Educators may have a long term condition, have a family member with a long term condition • Key Components • Identification of individuals willing to be lay educators • Development of programmes that are suitable for delivery by lay educators