Download
1 / 98
990 likes | 1.19k Views
Update on DSM-5 . MICHAEL J. LABELLARTE, SR., M.D. Annapolis, Millersville, Towson, and Columbia, MD dr.labellarte@cpeclinic.com cell:443-956-2463 www.cpeclinic.com. Tip of the Hat. Michael First, M.D. Master the Changes in the DSM-5 (TM). The Universe. School. Home. Everywhere Else.

E N D
Update on DSM-5 • MICHAEL J. LABELLARTE, SR., M.D. • Annapolis, Millersville, Towson, and Columbia, MD • dr.labellarte@cpeclinic.com • cell:443-956-2463 • www.cpeclinic.com
Tip of the Hat • Michael First, M.D. • Master the Changes in the DSM-5 (TM)
The Universe School Home Everywhere Else
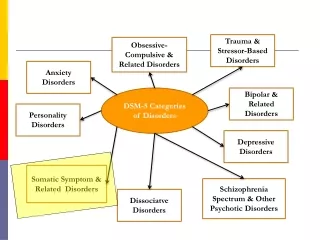
Outline • Preface • Highlights • Neurodevelopmental disorders • Other disorders of interest • Symptom/Disorder overlap
Whodunit? • Field Trials: large academic and small clinal centers • Work Groups • DSM-5 Task Forces • Review committees • APA Board of Trustees
DSM-5 Tidbits • Not obligatory to use DSM in U.S. • ICD-CM (“clinical modification”) is obligatory (HIPPA!) • Implementation of ICD-9 and ICD-10 (lands 10-1-14) • Incorporated into boards 2017 • “Online enhancements”: www.psych.org/dsm5
AXIS I-V Replaced • Non-axial documentation • Important psychosocial /contextual factors (V and Z codes) • Disability (may be replaced with the “WHODAS”) • GAF is eliminated
WHODAS • WHO Disability Assessment Schedule • “For further study” • Based on International Classification of Functioning, Disability, and Health (ICF) • A “useful” STD “measure of disability” • Designed for medical; presumptively “for mental disorders” • Child version not included
Elements of a Dx • Dx criteria • Dx subtypes and specifiers • Severity qualifiers are gone • Principal Dx • Provisional Dx - “strong presumption full criteria will be met”
DSM-5 Components • Section I • Section II • Section III • Appendices
Section I: Basics • Introduction • Use of the manual • Cautionary statement about forensics
Section II: Dx Criteria • Dx groupings of mental disorders • Medication-induced movement disorders/other adverse effects • Other conditions that may be a focus of clinical attention
Section II: Other ... • V codes and Z codes • Relational problems • “child affected by parental relationship distress” • Abuse and neglect • Etc.
Section III: Emerging • Assessment measures (e.g. WHODAS) • Cultural formulation • Alternative model for personality disorders • Conditions for further study
Appendices • Highlights of changes DSM-IV to DSM-5 • Glossary of technical terms • Glossary of cultural concepts of distress • Alphabetical and numerical listings of disorders
Mental Disorders:Metastructure I • Neurodevelopmental disorders: “intellectual disability”, global developmental delay, “ASD”, LDs, communication disorders (ex; social (pragmatic) communication disorder, ADHD, “motor disorders” • Schizophrenia spectrum and psychotic disorders: the usual, plus catatonia is expanded upon
Metastructure II • Bipolar and related disorders: includes “substance induced bipolar” • Depressive disorders: the usual plus DMDD (disruptive mood dysregulation disorder) and PMDD (premenstrual dysphoric disorder) • Bereavement exclusion eliminated from MDD
Metastructure III • Anxiety disorders: the usual • OCD and related disorders: body-dysmorphic disorder (BDD), hoarding, excoriation disorder, etc. • Trauma and stress-related disorders: PTSD, Acute SD, reactive attachment, disinhibited social engagement disorder, adjustment disorders
Metastructure IV • Dissociative disorders • Somatic symptom disorders • Feeding and eating disorders: AN, bulemia, binge eating disorder, avoidant/restrictive food intake, pica, rumination disorder • Elimination disorders
Metastructure V • Sleep/wake disorders: several new disorders ICSD including REM sleep behavior, restless leg syndrome • Sexual dysfunctions • Gender dysphoria
Metastructure VI • Disruptive, impulse control, and conduct disorders: ODD, CD, antisocial PD, pyromania, kleptomania, IED • Substance abuse and addictive disorders: substance use, substance induced, intoxication, withdrawal, gambling disorder • “Internet gaming disorder” in further research section (see appendix)
Metastructure VII • Neurocognitive disorders: delirium, major neurocognitive disorder, mild neurocognitive disorder • Personality Disorders • Paraphilias
Development • No clear distinction between child and adult disorders • Child specific disorders are relocated to appropriate sections • Groupings are etiology/risk/comorbidity, not age at dx • Disorders listed along “lifespan” (within groupings), ex. anxiety • Developmental modifications appropriate for Dx • Text includes “Development and Course”
Intellectual Disability • MR language is out • Clinical and STD IQ testing needed • Severity of impairment based on adaptive scores (not IQ): mild, moderate, severe, profound • Severity specifiers: conceptual, social, and practical domains
Global Developmental Delay • Akin to MR NOS • Age < 5 years, severity of ID cannot be reliably assessed • Unable to undergo systematic assessments
Autism Spectrum Disorder • Dimensional nature • Subsumes previous 5 types of PDD • Aspergers not distinct, but milder form of autism • False negatives could cause many w PDD to lose services • “Individuals with well-established DSM-IV dx” of PDD “should be given the dx of ASD”.
Autism Spectrum Disorder • Specifiers • Known med/gen/environ factor/other disorder • Severity (A, B): support, substantial, very substantial • If intelligence, if language, if catatonia
Autism Spectrum Disorder • A. Persistent deficits in social communication or social interaction across multiple contexts, current/by history (3/3) • 1. Social-emotional reciprocity • 2. Non-verbal communicative behavior used for social interaction • 3. Developing, maintaining, understanding relationships
Autism Spectrum Disorder • B. Restricted, repetitive behavior, interests, activities (2/4) • 1. Stereotyped or repetitive speech, motor movements, or use of objects • 2. Adherence to routines, ritualized patterns of verbal or non-verbal, or resistance to change • 3. Highly restricted, fixated interests (intense/focus) • 4. Hyper/hypo-reactivity to sensory input/aspects
Communication Disorders • Language disorders: combines expressive and expressive-receptive language disorders • Speech sound disorder (formerly phonological disorder) • Childhood-onset fluency disorder (formerly stuttering)
Social (Pragmatic) Communication Disorder • Persistent difficulty with verbal and non-verbal communication for social purposes (not better explained by ASD) • Previously PDD NOS
ADHD • Age of onset before age 12 • Age > 17: 5/9 symptoms diagnose • New (and better) text • Can officially be co-morbid with ASD
ADHD • Specifiers • In partial remission • Severity: mild, moderate, severe
ADHD Hallmarks • Inattention & Hyperactivity/Impulsivity • (Diagnostic criteria) • Frustration and negative emotionality • (DSM V Text)
ADHD DSM-5: Associated Features...Dx • “Tests of attention, executive function, or memory...are not sufficiently sensitive or specific to serve as diagnostic indices.” • “No biological marker is diagnostic for ADHD.”
Specific Learning Disorder • A single broader LD (subsumes the three Rs) • “Synthesis of history, school reports, and psycho-ed. testing.” • Impairment specifiers: reading, written expression, math • Ex.-word reading accuracy, grammar and punctuation accuracy, memorization of arithmetic facts (not just designate dyslexia or dyscalculia) • Severity specifier: mild, moderate, severe
Specific Learning Disorder • A. Difficulties learning and using academic skills (1/6, 6 mo) despite... provision of interventions... target those difficulties. • 1. Inaccurate/slow/effortful word reading • 2. Difficulty understanding meaning of what is read • 3. Difficulties with spelling • 4. Difficulties with written expression • 5. Difficulties mastering number sense, number facts, or calculation • 6. Difficulties with mathematical reasoning • 5
Motor Disorders • Developmental coordination disorder • Stereotypic movement disorder • Tic disorders
OTHER • Other specified neurodevelopmental disorder, e.g. FAE • Other unspecified neurodevelopmental disorder
Schizophrenia Spectrum • Schizotypal (personality) disorder • Delusional disorder • Brief psychotic disorder • Schizophreniform disorder • Schizophrenia • Schizoaffective disorder
Schizophrenia Spectrum • Schizophrenia: “bizarre”/Schneiderian AH do not stand alone • Schizophrenia subtypes are eliminated! • Delusional disorder: no longer just “non-bizarre” • Catatonia can be diagnosed with a specifier • 0-4 Severity ratings for psychosis (not included in desk ref)
Bipolar and Related • Bipolar I • Bipolar II • Cyclothymia
Bipolar Disorder • BPAD criteria same in children/adults • A. 1. mood disturbance (e.g elevated, expansive, irritable) and 2. increase in activity or energy • “Mixed episode” eliminated in BPAD I, but can be specified as “mixed features” • Duration: 4 days hypomania, 7 days mania; every day • Treatment-induced mania is “true mania”
Bipolar Disorder • B. 3/7 or 4/7 (if irritable mood) • 1. Inflated self-esteem grandiosity • 2. Decrease need for sleep • 3. More talkative/pressured speech • 4. Flights of ideas/racing thoughts • 5. Distractibility • 6. Goal directed activity/psychomotor agitation • 7. Increase... activities/painful consequences
Bipolar Disorder and Depressive Disorders • Specify: With anxious distress (2/5; m,m,m/s, s) • 1. Feeling keyed up/tense • 2. Feeling unusually restless • 3. Difficulty concentrating because of worry • 4. Fear that something awful may happen • 5. Feeling that the individual might lose control
BPAD vs. ADHD(Miller, Chiang, Ketter 2013) • FeatureBPADADHD • Age adoles./adult <12 yo • Gender M=F M>F • Course episodic persistent • Suicidal common rare • Psychotic “ “ • Euphoria “ “ • Less need sleep “ “ • Grandiose “ “ • Hypersexuality “ “ 25
Depressive Disorders • DMDD • Major depressive disorder (MDD) • Persistent depressive disorder (Dysthymia) • Premenstrual dysphoric disorder (PMDD)
Disruptive Mood Dysregulation Disorder (DMDD) • Controversial • Grouped with depressive disorders, not bipolar disorders • “Cannot coexist” with ODD, IED, or BPAD
DMDD • A. Severe recurrent temper outbursts manifested verbally (e.g. verbal rages) and/or behaviorally (e.g. physical aggression toward people or property) ... grossly out of proportion in intensity or duration to situation/provocation • B. Inconsistent with developmental level. • C. Frequency: tantrums on average >3 /week.