Download
1 / 57
570 likes | 686 Views
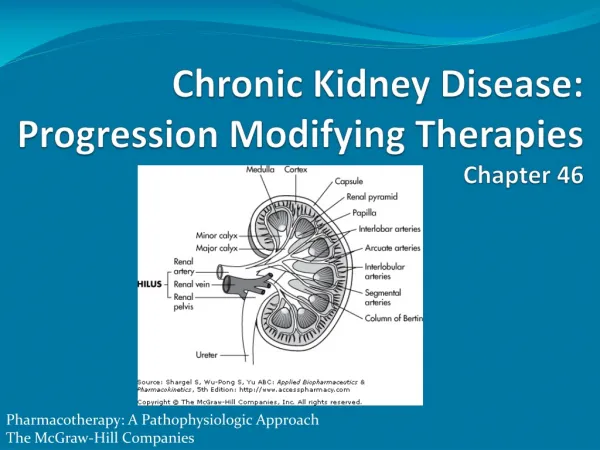
Improving Blood Pressure Treatment in the Community: Implications of the JNC7 Recommendations and ALLHAT Results Nathan D. Wong, PhD, FACC Professor and Director Heart Disease Prevention Program University of California, Irvine. Hypertension: A Significant CV and Renal Disease Risk Factor. CAD.

E N D
Improving Blood Pressure Treatment in the Community: Implications of the JNC7 Recommendations and ALLHAT Results Nathan D. Wong, PhD, FACCProfessor and DirectorHeart Disease Prevention ProgramUniversity of California, Irvine
Hypertension: A Significant CV and Renal Disease Risk Factor CAD CHF LVH Stroke Hypertension Renal disease Morbidity Disability Peripheral vascular disease National High Blood Pressure Education Program Working Group. Arch Intern Med. 1993;153:186-208.
Hypertension: How Big Is the Problem? At Least 65 Million Americans Require Treatment for Hypertension Nearly 1 in 3 adults (31%) in the US has hypertension Fields LE et al. Hypertension. 2004;44:398-404.
Men Women Men Women Men Women Men Women Risk of Cardiovascular Events by Hypertensive Status 36-Year Follow-up in Patients Aged 35-64 Years Peripheral Arterial Disease Cardiac Failure Coronary Disease Stroke 50 45.4 40 Normotensive Hypertensive Biennial Age-Adjusted Rate per 1,000 30 22.7 21.3 20 13.9 12.4 9.9 9.5 7.3 10 6.2 6.3 5.0 3.5 3.3 2.4 2.1 2.0 0 Reprinted with permission from Kannel WB. JAMA. 1996;275:1571-1576.
SBP-Associated Risks: MRFIT SBP versus DBP in Risk of CHD Mortality 80.6 48.3 CHD Death Rate 37.4 43.8 34.7 31.0 38.1 25.5 23.8 24.6 25.3 25.2 16.9 20.6 24.9 13.9 12.8 10.3 11.8 12.6 160+ 100+ 11.8 8.8 90–99 140–159 8.5 80–89 9.2 Diastolic BP(mm Hg) Systolic BP(mm Hg) 75–79 120–139 70–74 <120 <70 Adapted from Neaton JD et al. Arch Intern Med. 1992;152:56-64.
Distribution of Hypertension Subtype in the untreated Hypertensive Population in NHANES III by Age ISH (SBP ³140 mm Hg and DBP <90 mm Hg) SDH (SBP ³140 mm Hg and DBP ³90 mm Hg) IDH (SBP <140 mm Hg and DBP ³90 mm Hg) 100 80 60 40 20 0 17% 16% 16% 20% 20% 11% Frequency of hypertension subtypes in all untreated hypertensives (%) <40 40-49 50-59 60-69 70-79 80+ Age (y) Numbers at top of bars represent the overall percentage distribution of untreated hypertension by age. Franklin et al. Hypertension 2001;37: 869-874.
Elevated SBP Alone Is Associated With Increased Risk of Cardiovascular and Renal Disease Disease Relative Risk Kidney failure (ESRD) 2.8 Stroke 2.7 Heart failure 1.5 Peripheral vascular disease 1.8 Myocardial infarction* =1.6 Coronary artery disease 1.5 ESRD = end-stage renal disease; SBP 165 mm Hg. *Men only. Adapted from Kannel WB. Am J Hypertens. 2000;13:3S-10S; Perry HM Jr et al. Hypertension. 1995;25(part 1):587-594; Klag MJ et al. N Engl J Med. 1996;334:13-18; Nielsen WB et al. Ugeskr Laeger. 1996;158:3779-3783; Neaton JD et al. Arch Intern Med. 1992;152:56-64.
Prevalence, Awareness, Treatment, and Control of Hypertension in US Adults 2003-2004 (Ong et al., Hypertension 2007; 49: 69-75)
Prevalence (%) of HTN in US Adults, by Disease Status (Wong et al, Arch Intern Med 2007, in press) ** ** ** ** ** ** ** ** Mean age (y): 53.5 59.3 54.8 60.5 76.1 65.9 68.2 69.3 67.2 **P<0.01 when compared to No-Disease Group
Treatment (%) of HTN in US Adults, by Disease Status (Wong et al., Arch Intern Med 2007, in press) ** ** ** ** *P<0.05, **P<0.01 when compared to No-Disease group Treatment is in persons with HTN
Control (all treated) (%) of HTN in US Adults, by Disease Status (Wong et al., Arch Intern Med 2007, in press) * ** ** ** **P<0.05**P<0.01 when compared to No-Disease Group Control is in persons with HTN defined as BP < 140/90 If DM and CKD is based on BP<130/80 control is **35.3% and **23.2%, respectively. If MetS is based on BP<130/85 control is **46.7%
Mean BP and Distance to Goal Among HTN Pts Not at Goal (Wong et al., Arch Intern Med 2007, in press) Minimum BP distance from goal of < 140/90 in parenthesis, even with DM & CKD *p<0.05 **p<0.01 compared to no disease
4-Year Progression To Hypertension: The Framingham Heart Study Participants age 36 and older (<120/80 mm Hg) (130/85 mm Hg) (130-139/85-89 mm Hg) Vasan, et al. Lancet 2001;358:1682-86
HOT Study: Significant Benefit FromIntensive Treatment in the Diabetic Subgroup 25 20 Major cardiovascular events/1,000 patient-years 15 p=0.005 for trend 10 5 0 mm Hg 90 85 80 Target Diastolic Blood Pressure Hansson L et al. Lancet. 1998;351:1755-1762.
Benefits of Lowering BP Average Percent Reduction Stroke incidence 35–40% Myocardial infarction 20–25% Heart failure 50% TROPHY Study ACC 2006: Even lowering BP in those with pre-HTN appears to reduce incidence of new HTN by up to 60%
Preventable CHD Events from Control of Hypertension in US Adults(Wong et al., Am Heart J 2003; 145: 888-95) PAR% = population attributable risk (proportion of CHD events preventable), NNT = number needed to treat to prevent 1 CHD event ; <0.01 comparing men and women for PAR%
ALLHAT Randomized Designof ALLHAT Amlodipine Chlorthalidone Doxazosin Lisinopril High-risk hypertensive patients Consent / Randomize (42,418) Eligible for lipid-lowering Not eligible for lipid-lowering Consent / Randomize (10,355) Pravastatin Usual care Follow for CHD and other outcomes until death or end of study (up to 8 yr).
ALLHAT Baseline Characteristicsand Follow-up
ALLHAT Doxazosin Arm Terminated Early • Futility of finding a significant difference for primary CHD outcome • Statistically significant 20 percent higher rate of major secondary endpoint, combined CVD outcomes (80% higher rate of heart failure) Hypertension. 2003;42:239-246.
ALLHAT BP Results by Treatment Group Compared to chlorthalidone: SBP significantly higher in the amlodipine group (~1 mm Hg) and the lisinopril group (~2 mm Hg). Compared to chlorthalidone: DBP significantly lower in the amlodipine group (~1 mm Hg), similar in the lisinopril group.
ALLHAT .2 .16 .12 Cumulative CHD Event Rate .08 .04 0 0 1 2 3 4 5 6 7 Years to CHD Event Cumulative Event Rates for the Primary Outcome (Fatal CHD or Nonfatal MI) by ALLHAT Treatment Group Chlorthalidone Amlodipine Lisinopril
ALLHAT Subgroup Comparisons Results were consistent across age, race, gender, and baseline diabetes subgroups, except: • Stroke • Black L/C RR (95% CI) = 1.40 (1.17 – 1.68) • Non-Black L/C RR (95% CI) = 1.00 (0.85 – 1.17) • Combined CVD • Black L/C RR (95% CI) = 1.19 (1.09 – 1.30) • Non-Black L/C RR (95% CI) = 1.06 (1.00 – 1.13)
ALLHAT Total 0.98 (0.90, 1.07) Total 0.99 (0.91, 1.08) Age <65 0.99 (0.85, 1.16) Age < 65 0.95 (0.81, 1.12) Age>=65 0.97 (0.88, 1.08) Age >= 65 1.01 (0.91, 1.12) Men 0.98 (0.87, 1.09) Men 0.94 (0.85, 1.05) Women 0.99 (0.85, 1.15) Women 1.06 (0.92, 1.23) Black 1.01 (0.86, 1.18) Black 1.10 (0.94, 1.28) Non-Black 0.97 (0.87, 1.08) Non-Black 0.94 (0.85, 1.05) Diabetic 0.99 (0.87, 1.13) Diabetic 1.00 (0.87, 1.14) Non-Diabetic 0.97 (0.86, 1.09) Non-Diabetic 0.99 (0.88, 1.11) 0.50 1 2 0.50 1 2 Amlodipine Better Chlorthalidone Better Lisinopril Better Chlorthalidone Better Nonfatal MI + CHD Death – Subgroup Comparisons – RR (95% CI)
Predicted Cause-specific Mortalityfor 2 mm Hg lower SBP CHD -4 to -7% Stroke -4 to -10% Heart failure -5 to -7% Higher numbers for younger hypertensives Prospective Studies Collaboration, Lancet 2002;360:1903-13
ALLHAT 0.50 1 2 0.50 1 2 Lisinopril Chlorthalidone Better Better Amlodipine Chlorthalidone Better Better Summary of Outcomes Relative Risks and 95% CI
ALLHAT Fasting Glucose Results * p<.05 compared to chlorthalidone
ALLHAT ALLHAT Results by Baseline Diabetic Status • Outcome results were similar in diabetic and nondiabetic participants • For both diabetic and nondiabetic participants, there were significant advantages for the diuretic arm
ALLHAT Effect of 2-Year Changes in Fasting Glucose on ALLHAT Endpoints(Cox Regressions Beginning at 2 Years)
Diuretics, Potassium,and Glucose • Based on 40+ years’ evidence, potassium depletion is a major factor relating thiazide treatment and abnormal glucose. • Both reduced insulin release and decreased insulin sensitivity have been demonstrated. • More attention than is often given to preventing or reversing hypokalemia is warranted, especially in patients at risk of diabetes. Reference: Wilcox CS. Seminars in Nephrology, 1999;19:557-68.
Large Hypertension Trials Comparing Two or More Regimens: CVD or CV Mortality Trial n BPΔ Outcomes CAPPP 10,985 +3/+1 captopril not superior to D/BB NORDIL 10,881 +3/0 diltiazem not superior to D/BB CONVINCE 16,602 0/+1 verapamil not superior to D/BB STOP-2 6,628 0/-1 isradipine/felodipine & 0/0 ACEIs not superior to D/BB INSIGHT 6,592 0/0 nifed GITS not superior to diuretic LIFE 9,193 +1/0 losartan superior to atenolol ANBP-2 6,083 +1/0 ACEIs not superior to diuretics ALLHAT 42,418 -3/-1 chlorthalidone superior to doxazosin, -1/+1,-2/ 0 amlodipine (HF only), lisinopril INVEST 22,576 0/ 0 verapamil (+trandolapril) equivalent to atenolol (+HCTZ) VALUE 15,313 +2/+2 valsartan not superior to amlodipine
Large, controlled trials have shown similar mortality or morbidity reductions with: Bendrofluazide (MRC) Chlorthalidone (SHEP, HDFP) Hydrochlorothiazide (VA, Oslo, Australian) Indapamide (PATS, PROGRESS) HCTZ/amiloride (MRC-O, STOP-H) HCTZ/triamterene (EWPHE) Conclusion Independent trial findings support the view that all thiazide diuretics are beneficial
ACEIs and ARBs Reduce Cardiovascular Morbidity and Mortality ACEIs ARBs Val-Heft CHARM-Added HOPE CONSENSUS SOLVD LIFE Placebo (n=1284) Enalapril (n=1285) Placebo (n=126) Enalapril (n=127) Placebo (n=4652) Ramipril (n=4645) Atenolol (n=4588)Losartan (n=4605) Placebo (n=1272) Candesartan (n=1276) Valsartan (n=2511) Placebo (n=2499) 0 –10 Relative Risk Reduction, % –20 Mortality in chronic HF Total mortalityin severe HF MI, stroke, or CV death in high-risk patients Death, MI, or stroke in patients aged 55–80 years with hypertension and LVH All cause mortality and morbidity in patients with HF CV death or HF hospitalizationin patients with chronic HF –30 –40 angiotensin-converting enzyme inhibitors (ACEI); angiotensin receptor blocker (ARB);myocardial infarction (MI); cardiovascular (CV); heart failure (HF); left ventricular hypertrophy (LVH). Yusuf S et al. N Engl J Med. 2000;342:145-153; The CONSENSUS Trial Study Group. N Engl J Med. 1987;316:1429-1435; The SOLVD Investigators. N Engl J Med. 1991;325:293-302; Granger CB et al. Lancet. 2003;362:772-776; Dahlof B et al. Lancet. 2002;359:995-1003; Cohn JN et al. N Eng J Med. 2001;345:1667-1675.
Implications for Your Practice and Your Patients • The blood pressure goal for most patients with hypertension is <140/90 mm Hg. • Initial drug therapy for most should be either thiazide-type diuretic alone or combined with other drug classes. • Most patients with uncontrolled Stage 1 or Stage 2 hypertension should experience better blood pressure control and better long term CVD risk when the medication regimen includes a thiazide-type diuretic.
Without Compelling Indications With Compelling Indications Drug(s) for the compelling indications Other antihypertensive drugs (diuretics, ACEI, ARB, BB, CCB) as needed. Stage 1 Hypertension(SBP 140–159 or DBP 90–99 mmHg) Thiazide-type diuretics for most. May consider ACEI, ARB, BB, CCB, or combination. Stage 2 Hypertension(SBP >160 or DBP >100 mmHg) 2-drug combination for most (usually thiazide-type diuretic and ACEI, or ARB, or BB, or CCB) Not at Goal Blood Pressure Optimize dosages or add additional drugs until goal blood pressure is achieved.Consider consultation with hypertension specialist. Algorithm for Treatment of Hypertension Lifestyle Modifications Not at Goal Blood Pressure (<140/90 mmHg) (<130/80 mmHg for those with diabetes or chronic kidney disease) Initial Drug Choices
AHA Scientific Statement Recommendations: General CVD Prevention, High CAD Risk, Stable and Unstable Angina, NSTEMI, STEMI, LVD (Circulation 2007; 115: 2761-2788)
AHA 2007 Statement Recommendations • A target BP of <130/80 mmHg is reasonable for individuals with any of the following (Class IIa, level of evidence B): • Diabetes mellitus • Chronic renal disease • Coronary artery disease (CAD) • CAD risk equivalents • Carotid artery disease • Peripheral artery disease • Abdominal aortic aneurysms • High risk pts defined as >=10% 10-year risk from FRS
Renin Inhibition With AliskirenBinding of Angiotensinogen Prevented Aliskiren binds to a pocket in the renin molecule, blocking angiotensinogen from being cleaved by renin • Angiotensinogen Rahuel J et al. J Struct Biol. 1991;107:227-236.
Non-ACEpathways Aliskiren ACE ACEIs (Pro)Reninreceptor Heart Kidney Aldosterone Vessels • Vasoconstriction • Remodelling Ang III + IV Aliskiren Suppresses the Entire System—Targets the Point of Activation Aliskiren • (Pro)Renin Receptor • Actions: • Binding of (Pro)Renin • Increased renin catalytic activity • Activates VSMC ERK1/2 Angiotensinogen Renin Ang I Ang II Target cell ARBs AT1 receptor renin-angiotensin-aldosterone system (RAAS); vascular smooth muscle cells (VSMC); extracellular singal-regulated kinases (ERK 1/2); angiotensin (Ang); angiotensin-converting enzyme (ACE); angiotensin-converting enzyme inhibitor (ACEI); angiotensin receptor blockers (ARB); type 1 angiotensin II receptor (AT1) .
Lifestyle Modifications • Most patients will experience better control if they modify diet and exercise. • Physician advice sometimes works and should always be given along with a follow-up visit appointment to monitor both blood pressure and lifestyle change efforts. • Most of us do not do lifestyle counseling beyond simple advice and admonishment – the time factor is a problem. • Nevertheless, lifestyle modification is at the top of the JNC7 algorithm.
Keys to Physician Influence in Lifestyle Modification • Advice giving and follow-up monitoring are a minimum (many pts are not adequately titrated to goal BP) • Some evidence that brief behavioral counseling aimed at matching messages to patient readiness to change and eliciting the patient’s own motivation to change can move the patient along a continuum of change
Physician Influence in Lifestyle Modification- What to DoPICM • Permission: Ask the patient for permission to talk about lifestyle change and get preference for beginning with diet or exercise • Interest: Ask the patient about readiness to change – How interested are you on a scale of 1-10. Ask why they are not a lower number – to elicit a motivational statement from the patient. • Confidence: Ask how sure they are that they can do the behavior – again ask why not a lower number • Match a message to interest and confidence