Download
1 / 46
460 likes | 597 Views
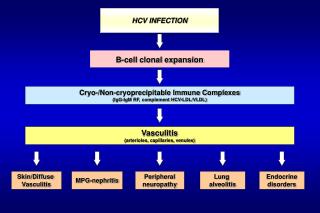
Best of HCV from EASL. Savino Bruno, MD Milano, Italy. This activity is supported by an independent medical education grant from AbbVie , Bristol-Myers Squibb and Gilead Sciences. Abstract #O7.

E N D
Best of HCV from EASL Savino Bruno, MD Milano, Italy This activity is supported by an independent medical education grant from AbbVie, Bristol-Myers Squibb and Gilead Sciences
Abstract #O7 Once-Daily Simeprevir (TMC435) Plus Sofosbuvir (GS-7977) With or Without Ribavirin in HCV Genotype 1 Prior Null Responders With Metavir F0-2: Cosmos Study Subgroup Analysis M. Sulkowski1, I.M. Jacobson2, R. Ghalib3, M. Rodriguez-Torres4, Z. Younossi5, A. Corregidor6, B. Fevery7, K. Callewaert8, W. Symonds9, G. De La Rosa10, G. Picchio11, S. Ouwerkerk-Mahadevan8, T. Lambrecht12, E. Lawitz13 1Johns Hopkins University School of Medicine, Baltimore, MD, 2Weill Cornell Medical College, New York, NY, 3Texas Clinical Research Institute, Arlington, TX, 4Fundaci_n de Investigaci_n, San Juan, PR, 5Department of Internal Medicine, Inova Fairfax Hospital, Falls Church, VA, 64800 Belfort Rd, Jacksonville, FL, United States, 7Janssen Research & Development, Janssen Infectious Diseases BVBA, Beerse, Belgium, 8Janssen Research & Development, Beerse, Belgium, 9Gilead Sciences, Inc., Foster City, CA, 10Janssen Global Services, Raritan, NJ, United States, 11Novellas Healthcare, Zellick, Belgium, 12Janssen Research & Development, Titusville, NJ, 13The Texas Liver Institute, University of Texas Health Science Center, San Antonio, TX, United States
COSMOS Study Design: Randomised, Multicentre, Open-label Trial • Cohort 1: METAVIR F0-F2, prior null responders to PR therapy • Stratified by IL28B, HCV GT 1 subtype • Primary endpoint: SVR12 • Secondary endpoints included RVR and relapse rate 0 4 12 24 36 48 Week Arm 1 SMV + SOF + RBV Post-treatment follow-up Randomised 2:1:2:1 Arm 2 SMV + SOF Post-treatment follow-up SMV + SOF + RBV Arm 3 Post-treatment follow-up Arm 4 SMV + SOF Post-treatment follow-up SMV 150 mg QD + SOF 400 mg QD±RBV 1000/1200 mg/day (BID) BID, twice daily; GT, genotype; QD, once daily; RBV, ribavirin; RVR, rapid virologic response; SMV, simeprevir; SOF, sofosbuvir; SVR12, sustained virologic response 12 weeks after end of treatment Sulkowski, M. et al. EASL 2014, Abstract #O7
COSMOS Cohort1: SVR12 – Primary endpoint (ITT population) 12 weeks 24 weeks 100 100 1/27 1/24 1/15 1/14 4/24 80 80 SVR12 60 60 Non-VF Proportion of patients(%) Relapse 40 40 20 20 19/24 14/15 26/27 13/14 0 0 SMV/SOF + RBV SMV/SOF SMV/SOF + RBV SMV/SOF ITT, intent-to-treat; Non-VF, Non-virologicfailure, patients who did not achieve SVR12 for reasons other than virologic failure Sulkowski, M. et al. EASL 2014, Abstract #O7
COSMOS Cohort 2: SVR12 by HCV GT 1 Subtype and Baseline NS3 Q80K Polymorphism (Excluding Non-VF*) SVR12 (%) 4/4 7/7 8/9 3/3 7/7 3/3 6/6 12/12 8/9 4/4 4/4 5/6 17/17 30/30 24/27 SMV/SOF + RBV SMV/SOF SMV/SOF + RBV SMV/SOF SMV/SOF±RBV 24 weeks Overall 12 weeks *Excluding patients who discontinued for non-virologic reasons Sulkowski, M. et al. EASL 2014, Abstract #O7
Conclusions • SMV/SOF QD led to high SVR12 rates in HCV GT1-infected patients regardless of treatment duration or the addition of RBV • SVR12 rates were high, regardless of baseline characteristics: • HCV GT1 subtype, Q80K polymorphism, IL28B genotype • On-treatment virologic response, including RVR, was not predictive of SVR • Two Phase 3 trials investigating SMV/SOF without ribavirin are ongoing (OPTIMIST-1 and -2) GT, genotype; ITT, Intent-to-treat; QD, once daily; RBV, ribavirin; SMV, simeprevir; SOF, sofosbuvir; SVR12, sustained virologic response 12 weeks after end of treatment Sulkowski, M. et al. EASL 2014, Abstract #O7
Abstract #O165 SimeprevirPlus Sofosbuvir With/Without Ribavirin inHCV Genotype-1 Prior Null-responder / Treatment-naïve Patients (COSMOS Study): Primary Endpoint (SVR12) Results in Patients With METAVIR F3-4 (Cohort 2) E. Lawitz1, R. Ghalib2, M. Rodriguez-Torres3, Z.M. Younossi4, A. Corregidor5, M.S. Sulkowski6,E. DeJesus7, B. Pearlman8, M. Rabinovitz9, N. Gitlin10, J.K. Lim11, P.J. Pockros12, B. Fevery13,T. Lambrecht14, S. Ouwerkerk-Mahadevan13, K. Callewaert13, W.T. Symonds15, G. Picchio16,K. Lindsay16, M. Beumont-Mauviel13, I.M. Jacobson17 1Texas Liver Institute, San Antonio, 2Medicine and Gastroenterology and Hepatology, The Liver Institute, Dallas, TX, 3Fundacion de Investigacion, San Juan, PR, 4Department of Medicine, Inova Fairfax Hospital, Falls Church, VA, 5Borland-Groover Clinic, 4800 Belfort Rd, Jacksonville, FL, 6Johns Hopkins University School of Medicine, Baltimore, MD, 7Orlando Immunology Center, Orlando, FL, 8Atlanta Medical Center, Atlanta, GA, 9University of Pittsburgh Medical Center, Pittsburgh, PA, 10Atlanta Gastroenterology Association, Atlanta, GA, 11Yale School of Medicine, New Haven, CT, 12Scripps Clinic, La Jolla, CA, United States, 13Janssen Research & Development, Beerse, 14Novellas Healthcare, Zellik, Belgium, 15Gilead Sciences Inc, Foster City, CA, 16Janssen Research & Development LLC, Titusville, NJ, 17Weill Cornell Medical College, New York, NY, United States
COSMOS Cohort 2: SVR12 – Primary Endpoint (ITT population) SVR12 Non-VF Relapse 3/87 3% 2/30 2/27 1/14 2% 2/87 Proportion of patients (%) 93% 100% 93% 93% 94% 28/30 16/16 25/27 13/14 82/87 SMV/SOF + RBV SMV/SOF SMV/SOF + RBV SMV/SOF SMV/SOF±RBV Non-VF, patients who did not achieve SVR12 for reasons other than virologic failure ITT, intent-to-treat; Non-VF, Non-virologic failure; RBV, ribavirin; SMV, simeprevir; SOF, sofosbuvir; SVR12, sustained virologic response 12 weeks after planned treatment end BID, twice daily; GT, genotype; QD, once daily; RBV, ribavirin; RVR, rapid virologic response; SMV, simeprevir; SOF, sofosbuvir; SVR12, sustained virologic response 12 weeks after end of treatment Lawitz, E. et al. EASL 2014, Abstract #O165 24 weeks Overall 12 weeks
COSMOS Cohort 2: SVR12 by HCV GT 1 Subtype and Baseline NS3 Q80K Polymorphism (Excluding Non-VF*) 100 100 100 100 100 100 100 100 GT 1b GT 1a without Q80K GT 1a with Q80K 100 96 88 100 100 95 93 80 88 60 SVR12 (%) 40 20 0 6/6 11/11 11/11 4/4 7/7 4/4 5/5 13/14 7/8 3/3 7/8 3/3 18/18 38/40 25/26 SMV/SOF + RBV SMV/SOF SMV/SOF + RBV SMV/SOF SMV/SOF±RBV 24 weeks Overall 12 weeks GT, genotype; non-VF, non-virologic failure; RBV, ribavirinSMV, simeprevir; SOF, sofosbuvir; SVR12, sustained virologicresponse 12 weeks after planned treatment end Lawitz, E. et al. EASL 2014, Abstract #O165 *Excluding patients who discontinued for non-virologic reasons
Conclusions • SMV/SOF QD led to SVR12 rates of 93-100% (ITT) in HCV GT 1 infected treatment-naïve and prior null-responder patients with METAVIR F3-4 • SVR12 rates were high, regardless of baseline characteristics: • HCV GT 1 subtype, Q80K polymorphism, METAVIR score,IL28B GT, prior treatment history • SMV/SOF QD +/- RBV was safe and well tolerated • Two Phase 3 trials investigating SMV/SOF without RBV are ongoing (OPTIMIST-1 and -2) Lawitz, E. et al. EASL 2014, Abstract #O165
Abstract #O68 Sofosbuvirand Ribavirin for the Treatment of Chronic HCV With Cirrhosis and Portal Hypertension With and Without Decompensation: Early Virologic Response and Safety Nezam Afdhal,1 Gregory Everson,2 Jose Luis Calleja,3 Geoffrey McCaughan,4 William T. Symonds,5 Diana Brainard,5 Jill Denning,5 Theo Brandt-Sarif,5 Lindsay McNair,5 John G. McHutchison,5Sarah Arterburn,5 Jaime Bosch,10 Michael Charlton,6Rajender Reddy,7Tarik Asselah,8 Edward Gane,9 Xavier Forns10 1Beth Israel Deaconess Medical Center, Boston, MA, USA; 2University of Colorado Denver, Aurora, CO, USA; 3Hospital Puerta de Hierro, Madrid, Spain; 4Royal Prince Alfred Hospital, University of Sydney, New South Wales, Australia; 5Gilead Sciences, Inc., Foster City, CA, USA; 6Mayo Clinic, Rochester, MN, USA;7University of Pennsylvania, Philadelphia, PA, USA; 8Hopital Beaujon, INSERM U 773 and University Paris-Diderot, Clichy, France; 9Auckland City Hospital, Grafton, Auckland, New Zealand; 10Hospital Clinic, Institutd’InvestigacionsBiomèdiques August Pi iSunyer, and Centro de InvestigaciónBiomédica en Red de EnfermedadesHepáticas y Digestivas, Barcelona, Spain
Study Design and Aim • Aim: To explore the safety and efficacy of SOF+RBV in HCV-infected patients with portal hypertension ± decompensated liver disease • Primary objective: SVR12 • Secondary objectives • Effects of 48 weeks of treatment on hepatic portal pressure and function • Safety and clinical improvement as measured by clinical outcomes, CPT, MELD, and biochemical test results Wk24 Wk48 Wk72 Wk96 Wk 0 HVPG at Day 0 and Week 48 SVR 12 SOF 400 mg + RBV 1000-1200 mg Arm 1 N=25 HVPG at Day 0, and Weeks 24 and 72 SVR 12 Observation SOF 400 mg + RBV 1000-1200 mg Arm 2 N=25 Study results through the first 24 weeks are presented Afdhal, N. et al. EASL 2014, Abstract #O68
Results: Virologic Response on Treatment 5/9 7/16 9/9 12/16 8/8 15/16 8/8 15/16 7/7 14/15 *1 patient was a non-responder at Week 8. Afdhal, N. et al. EASL 2014, Abstract #O68
Conclusions • In HCV-infected patients with portal hypertension with and without hepatic decompensation, treatment with SOF+RBV for up to 24 weeks resulted in: • High rates of virologic suppression irrespective of severity of liver disease • Decreased necroinflammation with ALT normalization • Improvements in platelet count and albumin • Improvement in ascites and hepatic encephalopathy • SOF+RBV for up to 24 weeks was generally safe and well tolerated with low rates of treatment discontinuation due to AEs • No patients developed worsening or new onset hepatic decompensation Afdhal, N. et al. EASL 2014, Abstract #O68
Abstract #O6 Sofosbuvir/Ledipasvir Fixed Dose Combination is Safe and Effective in Difficult-to-treat Populations Including Genotype-3 Patients, Decompensated Genotype-1 Patients, and Genotype-1 Patients With Prior Sofosbuvir Treatment Experience E.J. Gane1, R.H. Hyland2, D. An2, P.S. Pang2, W.T. Symonds2, J.G. McHutchison2, C.A. Stedman3 1Auckland Clinical Studies, Auckland, New Zealand; 2Gilead Sciences, Inc., Foster City, CA, United States; 3Christchurch Clinical Studies Trust, Christchurch, New Zealand
ELECTRON-2: Study Design • HCV GT 1, relapsed after previous treatment with SOF-containing regimens in ELECTRON-1 • HCV GT 1 decompensated cirrhosis (Child Pugh Turcotte B) • HCV GT 3, treatment naïve Wk 12 Wk 24 Wk 0 SVR12 GT 1Prior SOF exposure LDV/SOF+ RBV, n=19 GT 1CPT class B LDV/SOF, n=20 GT 3Treatment naïve LDV/SOF, n=25 Randomized LDV/SOF + RBV, n=26 Gane, E. et al. EASL 2014, Abstract #O6
ELECTRON-2 Results:(1) Prior Sofosbuvir-Treated GT 1 Patients • All 19 previous SOF-regimen failures had relapsed Re-treatment SOF+RBV 12 wk Prior Null Responders SOF+RBV 12 wk Treatment Naïve n=4 SVR12 (%) n=6 n=1 GS-9669 + SOF +RBV 12 wk Treatment Naïve LDV/SOF+RBV 6 wk Treatment Naïve n=8 19/19 19/19 Gane, E. et al. EASL 2014, Abstract #O6
ELECTRON-2 Results:(2) Patients With CPT B Cirrhosis 7 relapsers SVR12 (%) 13/20 Error bar represents the 95% confidence interval. Gane, E. et al. EASL 2014, Abstract #O6
ELECTRON-2 Results:(3) Patients With HCV GT 3, Treatment Naïve 100 100 64* 80 60 SVR12 (%) 40 20 16/25 26/26 16/25 26/26 0 LDV/SOF 12 Weeks LDV/SOF + RBV 12 Weeks *Failure due to relapse (n=8) or discontinuation due to AE (n=1) Gane, E. et al. EASL 2014, Abstract #O6
ELECTRON-2 Conclusions LDV/SOF regimens for 12 weeks are safe and effective IFN-free treatments for many diverse and difficult-to-treat patient populations including: • Patients infected with HCV GT 1 who have failed previous SOF-containing regimens • Patients infected with HCV GT 1 with decompensated cirrhosis • Patients infected with HCV GT 3 Gane, E. et al. EASL 2014, Abstract #O6
Abstract #O1 SAPPHIRE II: Phase 3 Placebo-Controlled Study Of Interferon-Free, 12-Week Regimen Of ABT-450/r/ABT-267, ABT-333, And Ribavirin In Treatment-Experienced Adults With Hepatitis C Virus Genotype 1 S. Zeuzem1, I. Jacobson2, T. Baykal3, R.T. Marinho4, F. Poordad5, M. Bourliere6, M. Sulkowski7, H. Wedemeyer8, E. Tam9, P. Desmond10, D. Jensen11, A.M. Di Bisceglie12, P. Varunok13, T. Hassanein14, J. Xiong3, B. DaSilva-Tillmann3, L. Larsen3, T. Podsadecki3 1J.W. Goethe University, Frankfurt, Germany, 2Weill Cornell Medical College, New York, NY, 3AbbVie Inc., North Chicago, IL, United States, 4Centro Hospitalar de Lisboa Norte, Lisbon, Portugal, 5The Texas Liver Institute, University of Texas Health Science Center, San Antonio, TX, United States, 6Hopital Saint Joseph, Marseille, France, 7Johns Hopkins University, Baltimore, MD, United States, 8Medizinische Hochschule Hannover, Hannover, Germany, 9LAIR Centre, Vancouver, BC, Canada, 10St Vincent's Hospital (Melbourne), Fitzroy, VIC, Australia, 11Center for Liver Diseases, University of Chicago Medical Center Chicago, Chicago, IL, 12Saint Louis University, St. Louis, MO, 13Premier Medical Group of the Hudson Valley, PC, Poughkeepsie, NY, 14Southern California Liver Centers and Southern California Research Center, Coronado, CA, United States
SAPPHIRE-II: Placebo-Controlled Design (N=394) • 3D: co-formulated ABT-450/r/ombitasvir, 150 mg/100 mg/25 mg QD; dasabuvir, 250 mg BID • RBV: 1000-1200 mg daily according to body weight (<75 kg and >75kg, respectively) Open-Label Treatment Period Double-Blind Treatment Period 3D + RBV (n=297) 48-Week Follow-Up Placebo (n=97) 48-Week Follow-Up 3D + RBV Week 0 Week 12 Week 24 Week 60 Week 72 Primary Analysis: SVR12 Zeuzem, S. et al. EASL 2014, Abstract #O1
SAPPHIRE-II: Baseline Patient Characteristics *IL28B rs12979860 HCV genotype and subtype assessed using the Versant HCV Genotype Inno-LiPA Assay, v2.0. HCV RNA level measured by COBAS TaqMan real-time reverse-transcriptase–polymerase-chain-reaction assay, v2.0 (Roche). Zeuzem, S. et al. EASL 2014, Abstract #O1
SAPPHIRE-II Results: ITT SVR12 Rates (Superior to Placebo) 96.7% 96.0% 96.3% SVR12, % Patients 286/297 166/173 119/123 GT1a GT1b All Patients Zeuzem, S. et al. EASL 2014, Abstract #O1
SAPPHIRE-II Results: ITT SVR12 Rates >95% in All Prior PEG/RBV Response Groups 100% 95.3% 95.2% SVR12, % Patients 82/86 65/65 139/146 Prior Partial Response Prior Null Response Prior Relapse Zeuzem, S. et al. EASL 2014, Abstract #O1
SAPPHIRE-II: Conclusions • The ITT SVR12 rate was 96.3% (286/297) for treatment-experienced GT1-infected patients receiving 12 weeks of ABT-450/r/ombitasvir + dasabuvir + RBV • High SVR12 rates regardless of HCV subtype and across all prior pegIFN/RBV response groups • The regimen was generally well-tolerated, with a low rate of study drug discontinuation due to AE(s) (1.0%) Zeuzem, S. et al. EASL 2014, Abstract #O1
Abstract #O163 TURQUOISE-II:SVR12 Rate of 92-96% in 380 Hepatitis C Virus Genotype 1-infected Adults With Compensated Cirrhosis Treated With ABT-450/R/ABT-267 and ABT-333 Plus Ribavirin F. Poordad1, C. Hezode2, R. Trinh3, K.V. Kowdley4, S. Zeuzem5, K. Agarwal6, M.L. Shiffman7, H. Wedemeyer8, T. Berg9, E.M. Yoshida10, X. Forns11, S.S. Lovell3, B. Da Silva-Tillmann3, A.L. Campbell3, T. Podsadecki3 1The Texas Liver Institute/University of Texas Health Science Center, San Antonio, TX, United States, 2Henri Mondor Hospital, APHP, University Paris-Est, Inserm U955, Creteil, France, 3AbbVie Inc., North Chicago, IL, 4Digestive Disease Institute, Virginia Mason Medical Center, Seattle, WA, United States, 5J.W. Goethe University, Frankfurt, Germany, 6Institute of Liver Studies, Kings College Hospital, London, United Kingdom, 7Liver Institute of Virginia, Newport News, VA, United States, 8Medizinische Hochschule Hannover, Hannover, 9Universit_tsklinikum Leipzig, Leipzig, Germany, 10University of British Columbia, Vancouver, BC, Canada, 11Liver Unit, Hospital Clinic, IDIBAPS and CIBEREHD, Barcelona, Spain
TURQUOISE-II Study Design: Phase 3 Trial Conducted Exclusively in GT1-Infected Cirrhotic Patients (N=380) • 3D: co-formulated ABT-450/r/ombitasvir, 150 mg/100 mg/25 mg QD; dasabuvir, 250 mg BID • RBV: 1000-1200 mg daily according to body weight (<75 kg and >75kg, respectively) SVR12 3D + RBV (N=208) SVR12 3D + RBV (N=172) Day 0 Week 12 Week 24 Poordad, F. et al. EASL 2014, Abstract #O163
TURQUOISE-II:Demographics and Patient Characteristics 3D + RBV Poordad, F. et al. EASL 2014, Abstract #O163
TURQUOISE-II Results:ITT SVR12 Rates of 92% to 96% 95.9 P=0.089 91.8 SVR12, % Patients 191/208 165/172 12 Weeks 3D + RBV 24 Weeks 3D + RBV Poordad, F. et al. EASL 2014, Abstract #O163
TURQUOISE-II Results: ITT SVR12 Rates by Prior Treatment Response in HCV Subtype 1a 92.2 92.9 93.3 100 100 100 80.0 92.9 3D + RBV 12-week arm 24-week arm SVR12, % Patients 10/10 52/56 11/11 39/42 59/64 13/13 40/50 14/15 Prior Partial Response Prior Null Response Naïve Prior Relapse Response HCV Subtype 1a Poordad, F. et al. EASL 2014, Abstract #O163
TURQUOISE-II: Conclusions • First dedicated trial of IFN-free regimen in cirrhotic patients, including patients often ineligible for clinical trials (low platelets, low albumin, radiographic ascites) • SVR rates of 92% to 96% with 12 and 24 weeks of treatment, with high SVR rates in all subgroups analyzed • 12 or 24 weeks of treatment were similarly well tolerated, with low rates of treatment discontinuation • Efficacy and safety in this large cirrhotic population is similar to non-cirrhotics treated with the same regimen Poordad, F. et al. EASL 2014, Abstract #O163
Abstract #P1299 PEARL-III: 12 Weeks of ABT-450/R/267 + Abt-333 Achieved SVR in >99% of 419 Treatment-Naïve HCV Genotype 1b-Infected Adults With or Without Ribavirin P. Ferenci1, A. Nyberg2, P. Enayati3, D. Bernstein4, Y. Baruch5, F.A. Caruntu6, V. Chulanov7, E. Janczewska8, Z. Younes9, R.T. Marinho10, G.Rizzardini11, J. Gervain12, R. Planas13, C. Moreno14, W. Xie15, D.Cohen15, M. King15, T. Podsadecki15, K.R. Reddy16 1Universitaetsklinik fuerInnereMedizin III, Vienna, Austria, 2KaiserPermanente, San Diego, 3California Liver Institute, Los Angeles, 4North Shore University Hospital, Manhasset, CA, United States, 5Rambam Health Care Campus, Haifa, Israel, 6Institutul National de BoliInfectioase'Prof. Dr. MateiBals', Bucharest, Romania, 7Federal Budget Institute of Science Central Research Institute of Epidemiology, Moscow, Russian Federation, 8ID Clinic, Mysłowice, Poland,9GastroOne, Germantown, TN, United States, 10Centro HospitalarLisboa Norte, Lisboa, Portugal, 11Ospedale Luigi Sacco, Milano, Italy, 12Szent György Hospital, Székesfehérvár, Hungary, 13Hospital Germans TríasiPujol, CIBERehd, Badalona, Spain, 14CUB HôpitalErasme, UniversitéLibre de Bruxelles, Brussels, Belgium, 15AbbVie Inc., North Chicago, IL, 16University of Pennsylvania, Philadelphia, PA, United States
Figure 1 – PEARL III Study Design Assess for SVR12 48-wk Follow-up • All patients received the 3D regimen • ABT-450/r/ombitasvir: 150 mg/100 mg/25 mg QD • Dasabuvir: 250 mg BID • RBV 1000 mg if body weight was <75 kg, 1200 mg if body weight ≥75 kg (divided BID), or matching placebo Study drug dosing ABT-450/r/Ombitasvir + Dasabuvir + RBV 3D + RBV N = 210 ABT-450/r/Ombitasvir + Dasabuvir + Placebo for RBV 3D N = 209 Day 0 Week 12 Week 24 Week 60 Ferenci, P. et al. EASL 2014, Abstract #P1299
Figure 2. SVR12 Rates After 12 Weeks of 3D ± RBV 99.5 99.0 100 Superiority 84% 80 Noninferiority 73% 60 SVR12, % Patients 40 20 207/209 209/210 0 3D + RBV 3D Ferenci, P. et al. EASL 2014, Abstract #P1299
Conclusions • SVR12rates of 99.5% and 99% were achieved in treatment-naïve non-cirrhotic patients with GT1b infection following 12-week treatment with ABT-450/r/ombitasvir and dasabuvir with and without RBV, respectively • 1 of 419 patients experienced virologicfailure • No patient discontinued prematurely due to adverse events in either treatment group • Hematologic abnormalities and some adverse events were less frequent in the absence of RBV • The addition of RBV in this population did not provide additional clinical benefit
Abstract #O166 All-Oral Dual Therapy With Daclatasvirand Asunaprevir in Patients With HCV Genotype 1b Infection: Phase 3 HALLMARK-DUAL Study Results M. Manns1, S. Pol2, I. Jacobson3, P. Marcellin4, S. Gordon5, C.-Y. Peng6, T.-T. Chang7, G. Everson8, J. Heo9, G. Gerken10, B. Yoffe11, W.J. Towner12, M. Bourliere13, S. Metivier14, C.-J. Chu15, W. Sievert16, J.-P. Bronowicki17, D. Thabut18, Y.-J. Lee19, J.-H. Kao20, F. McPhee21, J. Kopit21, P. Mendez22, M. Linaberry22, E. Hughes22, S. Noviello22, HALLMARK DUAL Study Team 1Department of Gastroenterology, Hepatology and Endocrinology, Hannover Medical School, Hannover, Germany, 2H_pital Cochin, Paris, France, 3Weill Cornell Medical College, New York, NY, United States, 4Hopital Beaujon, Clichy, France, 5Henry Ford Health Systems, Detroit, MI, United States, 6School of Medicine, China Medical University, Taichung, 7National Chen Kung University Hospital, Tainan, Taiwan, 8University Of Colorado Denver, Aurora, CO, United States, 9Pusan National University Hospital, Busan, Korea, Republic of, 10University of Duisburg-Essen, Essen, Germany, 11VAMC, Baylor College of Medicine, Houston, TX, 12Kaiser Permanente, Los Angeles, CA, United States, 13Hopital Saint Joseph, Marseille, 14CHU Purpan, Toulouse, France, 15Taipei Veterans General Hospital and National Yang-Ming University, Taipei, Taiwan, 16Monash Health and Monash University, Melbourne, VIC, Australia, 17INSERM Unit_ 954, Centre HospitalierUniversitaire de Nancy and Universit_ de Lorraine, Vandoeuvre-l_s-Nancy, 18Hopital Piti_-Salp_tri_re, Paris, France, 19Inje University Busan Paik Hospital, Busan, Korea, Republic of, 20National Taiwan University Hospital, Taipei, Taiwan, 21Bristol-Myers Squibb Research and Development, Wallingford, CT, 22Bristol-Myers Squibb Research and Development, Princeton, NJ, United States
Global Phase 3 Study: HALLMARK-DUAL (AI447-028) • Primary endpoint: proportion of DCV + ASV-treated patients with SVR12 • Patients infected with HCV genotype 1b • Treatment-naïve • Nonresponders: prior null or partial response to pegIFN/RBV • Interferon-ineligible/intolerant (treatment-naïve or -experienced) due to • Depression • Anemia/neutropenia • Compensated advanced fibrosis/cirrhosis (F3/F4) with thrombocytopenia Week 12 Day 1 Week 24 Week 48 DCV 60 mg QD + ASV 100 mg BID 24 weeks(N = 203)a Follow up 24 weeks Randomization2:1 Treatment-naïve DCV-PBO + ASV-PBO 12 weeks (N = 102) Enter another study:DCV + ASV 24 weeks DCV + ASV 24 weeks(N = 205) Follow up 24 weeks Nonresponder DCV + ASV 24 weeks (N = 235) Follow up 24 weeks Ineligible/intolerant a Excludes 2 patients inadvertently assigned, instead of randomized, to DCV + ASV; patients were excluded from efficacy analyses but both achieved SVR12 SVR12 STOP Manns, M. et al. EASL 2014, Abstract #O166
Virologic Response: SVR12 SVR12 (% of patients)a,b 182/203 192/235 168/205 Treatment- naïve Nonresponders Ineligible/ intolerant • SVR12rates documented on or after posttreatment Week 12 • Treatment-naïve: 91% • Nonresponders: 82% • Ineligible/intolerant: 83% • a HCV RNA < lower limit of assay quantitation (25 IU/mL) • b Patients with missing SVR12 data counted as treatment failures • Manns, M. et al. EASL 2014, Abstract #O166
All-Oral Dual Therapy with Daclatasvir and Asunaprevirin Patients with HCV Genotype 1b Infection: A Phase 3 Study Results SVR12 (%) 88/111 113/142 104/124 153/171 182/203 192/235 55/63 168/205 29/32 Manns, M. et al. EASL 2014, Abstract #O166
Summary • All-oral DCV + ASV therapy achieved SVR12 rates up to 91% in treatment-naïve, 82% in nonresponder, and 83% in ineligible/intolerant patients with genotype 1b • SVR12 rates were similar in non-cirrhotic (85%) and cirrhotic (84%) patients • No differences by age, gender, race, IL28B genotype, or prior IFN/RBV treatment experience • DCV + ASV was generally safe and well tolerated • Only 2% of patients discontinued treatment due to adverse events • DCV is being further evaluated in all-oral combinations in multiple patient populations of high unmet need Manns, M. et al. EASL 2014, Abstract #O166
Abstract #O61 Efficacy and Safety of MK-5172 And MK-8742 ± RIBAVIRIN IN Hepatitis C Genotype 1 Infected Patients With Cirrhosis Or Previous Null Response: The C-WORTHY Study E. Lawitz1, C. Hezode2, E. Gane3, E. Tam4, M. Lagging5, L. Balart6, L. Rossaro7, R. Ghalib8, M. Shaughnessy9, P. Hwang9, J. Wahl9, M.N. Robertson9, B. Haber9 1The Texas Liver Institute, University of Texas Health Science Center, San Antonio, TX, United States, 2Department of Hepatology-Gastroenterology, Henri Mondor Hospital, University of Paris-Est, Creteil, France, 3Auckland Clinical Studies, Grafton, Auckland, New Zealand, 4LAIR Centre, Vancouver, BC, Canada, 5Department of Infectious Disease, Institute of Biomedicine, University of Gothenburg, Gothenburg, Sweden, 6Gastroenterology & Hepatology, Tulane University Medical Center, New Orleans, LA, 7Gastroenterology and Hepatology, University of California, Davis Medical Center, Sacramento, CA, 8Texas Clinical Research Institute, Arlington, TX, 9Merck, Whitehouse Station, NJ, United States
C-WORTHy:Treatment-Naïve Cirrhotics and Nulls • Aim: To assess the efficacy, safety and optimal treatment duration of MK-5172 + MK-8742 ±ribavirin in patients with HCV genotype 1 infection who are: • Treatment naïve with cirrhosis; or • Null responders to prior peginterferon/ribavirin (PR) ± cirrhosis • Key eligibility criteria: • Treatment-naïve patients ≥18 years old with chronic HCV GT1a or GT1b infection • Null response = <2 log10 decline from baseline in HCV RNA after 12 weeks of prior PR • Liver biopsy or noninvasive test • Minimum baseline hemoglobin: 12 g/dL (females) or 13 g/dL (males) • HIV and HBV negative • ALT and AST <350 IU/L • Albumin ≥3.0 g/dL; platelets ≥70,000/mm3 Treatment-naïve Non-cirrhotic 8-12 weeks ± RBV (n = 94) Treatment-naïve Cirrhotic 12-18 weeks ± RBV (n = 123) Null responders Cirrhotic / Non-cirrhotic 12-18 weeks ± RBV (n = 130) HIV/HCV co-infected Non-cirrhotic 12 weeks ± RBV (n = 59) Lawitz, E. et al. EASL 2014, Abstract #O61
Efficacy of MK-5172 + MK-8742 ± RBVin Treatment-Naïve Patients with Cirrhosis: 12 vs 18 Weeks 2831 31 31 29 30* 31 32 28 31 30 31 28 31 28 29 29 29 32 32 29 29 30 31* Breakthrough Relapse TW4 TW12 FU4/8 Discontinuation • *Excludes patients who have not yet reached the FU4 time point • 12 week arms include 97% of FU8 results Lawitz, E. et al. EASL 2014, Abstract #O61
Efficacy of MK-5172 + MK-8742 ± RBV in PR-Null Patients ± Cirrhosis: 12 vs 18 weeks 30 32 33 33 32 33 30 32 30 32 33 33 33 33 31 32 30 32 30 33 32 32* 29 30* Breakthrough Relapse TW4 TW12 FU4/8 Discontinuation • *Excludes patients who have not yet reached the FU4 time point • 12 week arms include 97% of FU8 results Lawitz, E. et al. EASL 2014, Abstract #O61
Summary/Conclusion Efficacy • MK-5172 + MK-8742 ± RBV demonstrated high efficacy: • 90-97% of cirrhotic patients achieved SVR4/8 • 91-100% of prior null responders achieved SVR4/8 • In treatment-naïve patients with cirrhosis, high efficacy was achieved regardless of use of RBV or extended treatment duration • In prior null-responder patients, a 12-week RBV-free regimen resulted in >90% SVR4/8 Safety • All treatment regimens were generally safe and well-tolerated These results support the ongoing Phase 3 development of MK-5172 + MK-8742 ± RBV in various patient populations Lawitz, E. et al. EASL 2014, Abstract #O61