Download
1 / 1
10 likes | 109 Views
Adjuvant chemotherapy in older women with breast cancer (AChEW): identifying perceptions and putative barriers in decision-making Lesley Fallowfield 1 , Helena Harder 1 , Carolyn Langridge 1 , Rachel Ballinger 1 , Alistair Ring 2

E N D
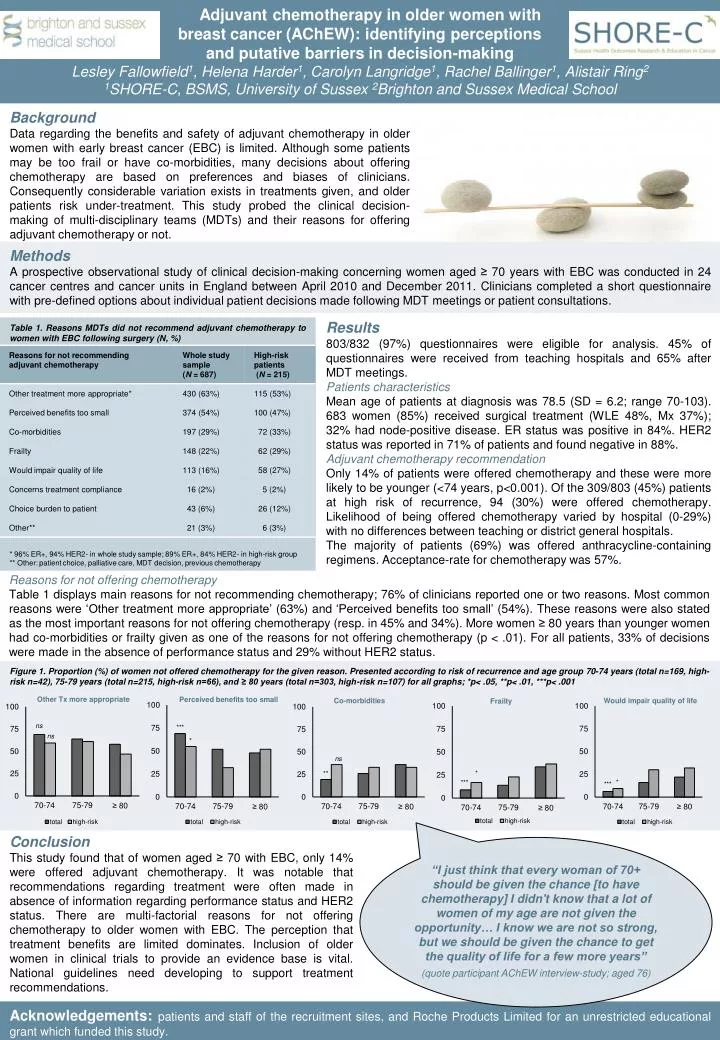
Adjuvant chemotherapy in older women with breast cancer (AChEW): identifying perceptions and putative barriers in decision-making Lesley Fallowfield1, Helena Harder1, Carolyn Langridge1, Rachel Ballinger1, Alistair Ring2 1SHORE-C, BSMS, University of Sussex 2Brighton and Sussex Medical School Background Data regarding the benefits and safety of adjuvant chemotherapy in older women with early breast cancer (EBC) is limited. Although some patients may be too frail or have co-morbidities, many decisions about offering chemotherapy are based on preferences and biases of clinicians. Consequently considerable variation exists in treatments given, and older patients risk under-treatment. This study probed the clinical decision-making of multi-disciplinary teams (MDTs) and their reasons for offering adjuvant chemotherapy or not. Methods A prospective observational study of clinical decision-making concerning women aged ≥ 70 years with EBC was conducted in 24 cancer centres and cancer units in England between April 2010 and December 2011. Clinicians completed a short questionnaire with pre-defined options about individual patient decisions made following MDT meetings or patient consultations. Results 803/832 (97%) questionnaires were eligible for analysis. 45% of questionnaires were received from teaching hospitals and 65% after MDT meetings. Patients characteristics Mean age of patients at diagnosis was 78.5 (SD = 6.2; range 70-103). 683 women (85%) received surgical treatment (WLE 48%, Mx 37%); 32% had node-positive disease. ER status was positive in 84%. HER2 status was reported in 71% of patients and found negative in 88%. Adjuvant chemotherapy recommendation Only 14% of patients were offered chemotherapy and these were more likely to be younger (<74 years, p<0.001). Of the 309/803 (45%) patients at high risk of recurrence, 94 (30%) were offered chemotherapy. Likelihood of being offered chemotherapy varied by hospital (0-29%) with no differences between teaching or district general hospitals. The majority of patients (69%) was offered anthracycline-containing regimens. Acceptance-rate for chemotherapy was 57%. Table 1. Reasons MDTs did not recommend adjuvant chemotherapy to women with EBC following surgery (N, %) * 96% ER+, 94% HER2- in whole study sample; 89% ER+, 84% HER2- in high-risk group ** Other: patient choice, palliative care, MDT decision, previous chemotherapy Reasons for not offering chemotherapy Table 1 displays main reasons for not recommending chemotherapy; 76% of clinicians reported one or two reasons. Most common reasons were ‘Other treatment more appropriate’ (63%) and ‘Perceived benefits too small’ (54%). These reasons were also stated as the most important reasons for not offering chemotherapy (resp. in 45% and 34%). More women ≥ 80 years than younger women had co-morbidities or frailty given as one of the reasons for not offering chemotherapy (p < .01). For all patients, 33% of decisions were made in the absence of performance status and 29% without HER2 status. Figure 1. Proportion (%) of women not offered chemotherapy for the given reason. Presented according to risk of recurrence and age group 70-74 years (total n=169, high-risk n=42), 75-79 years (total n=215, high-risk n=66), and ≥ 80 years (total n=303, high-risk n=107) for all graphs; *p< .05, **p< .01, ***p< .001 Conclusion This study found that of women aged ≥ 70 with EBC, only 14% were offered adjuvant chemotherapy. It was notable that recommendations regarding treatment were often made in absence of information regarding performance status and HER2 status. There are multi-factorial reasons for not offering chemotherapy to older women with EBC. The perception that treatment benefits are limited dominates. Inclusion of older women in clinical trials to provide an evidence base is vital. National guidelines need developing to support treatment recommendations. “I just think that every woman of 70+ should be given the chance [to have chemotherapy] I didn't know that a lot of women of my age are not given the opportunity… I know we are not so strong, but we should be given the chance to get the quality of life for a few more years” (quote participant AChEW interview-study; aged 76) Acknowledgements: patients and staff of the recruitment sites, and Roche Products Limited for an unrestricted educational grant which funded this study.