Download
1 / 40
400 likes | 560 Views
Risks of Ionizing Radiation, Contrast, and More in Diagnostic Imaging. Jon Hallstrom MS3 OHSU December 2006. Importance and Purpose. Diagnostic imaging has an expanding role and utility, and the management of nearly every inpatient is now affected by information obtained from imaging.

E N D
Risks of Ionizing Radiation, Contrast, and More in Diagnostic Imaging Jon Hallstrom MS3 OHSU December 2006
Importance and Purpose • Diagnostic imaging has an expanding role and utility, and the management of nearly every inpatient is now affected by information obtained from imaging. • In general, risks are quite low compared with potential benefit. However, many procedures are performed unnecessarily with risks of imaging and appropriateness guidelines neglected, in part due to overburdened health workers’ need for “time-efficient” care and growing medico-legal issues. • This presentation hopes to summarily identify and characterize risks associated with diagnostic imaging modalities with emphasis on radiation biology, or the study of effects of ionizing radiation, and adverse reactions to contrast agents.
Case Study—The Hulk1 • Created by Stan Lee and Jack Kirby, the Hulk first appeared in Marvel Comics’ Incredible Hulk # 1 (May 1962). • After nuclear physicist Dr. Robert Bruce Banner is caught in the blast of a gamma bomb he created, he is transformed into the Hulk, a raging monstrosity. • The Hulk possesses immense levels of physical strength… the Hulk's "capacity for physical strength is potentially limitless due to the fact that the Hulk's strength increases proportionally with his level of great emotional stress, anger in particular." • The Hulk's primary physical rival, the Abomination, is also gamma-spawned. He, like Bruce Banner, belongs to the small minority of people who are born with a genetic factor that cause them to change instead of being killed by the radiation. 1. From www.wikipedia.com “Hulk (Comics)”
Outline • Background Radiation • Ionizing Radiation • Physics and biology • Radiation Dose • Carcinogenesis • Hereditary consequences • Embryologic/Fetal effects • Contrast Media • MRI, Ultrasound
Background Radiation1 • Background radiation: • Estimated at 2.4mSv per year with a range of 1-10 • Approximately half is due to radon inhalation • Man-made radiation accounts for 18% of annual radiation exposure in the US, with medical X-rays and Gamma-rays accounting for 79% of artificial sources 1. Health Risks From Exposure to Low Levels of Ionizing Radiation: BEIR VII Phase 2 2006.
Background Radiation1 1. Health Risks From Exposure to Low Levels of Ionizing Radiation: BEIR VII Phase 2 2006.
Ionizing Radiation1,2,3 • Physics of Radiation • Diagnostic imaging utilizes X-rays and Gamma-rays, two forms of high energy, electromagnetic, indirectly-ionizing radiation • Ionization refers to the ability of X-rays or Gamma-rays, when absorbed by target tissues, to eject orbital electrons from an atom or molecule • 1. Hall’s Radiobiology for the Radiologist, Sixth Edition 2006. • 2. Health Risks From Exposure to Low Levels of Ionizing Radiation: BEIR VII Phase 2 2006. • 3. Fajardo’s Radiation Pathology 2001.
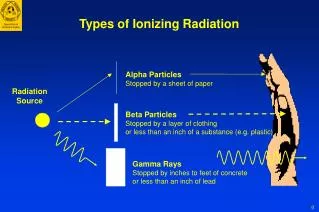
X-rays Artificially produced by anode bombardment of accelerated electrons in cathode ray tube Transmission radiation Used in radiography, including CT, angiography, fluoroscopy Gamma-rays Formed following electron capture or alpha or beta particle emission from unstable radionuclides Emission radiation Used in nuclear imaging studies Ionizing Radiation • X-rays and Gamma-rays may be considered identical for any given energy wavelength • X-rays and Gamma-rays are considered low linear transfer of energy (LET) radiation because they have a slow rate of energy transfer and are sparsely ionizing compared with particulate directly ionizing radiation
Ionizing Radiation X-rays being generated by anode bombardment of electrons? Actually, we are looking at the USS Enterprise, a galaxy class starship, entering warp speed.
Ionizing Radiation • Biology of X-rays and Gamma-rays • May directly ionize a target molecule or indirectly affect target molecules by free radical formation with propagation • Effects may extend beyond irradiated cells, particularly via intercellular gap junctions, known as the “bystander effect” • Genomic damage consists of chromosomal aberrations, instability, and gene mutations • Degree of damage may be affected by stage of cell cycle, hypersensitivity (eg hypoxic states), and protective agents (eg antioxidants) • Cells may attempt repair (eg DNA excision repair) or undergo apoptosis, but are not always successful
Ionizing Radiation • Radiation Dose • Absorbed dose: the ratio of energy imparted to the mass of the exposed body or organ, measured in gray (Gy = J/kg) • Equivalent dose: Accounts for variation in the degree of tissue damage created by different types of radiation (eg alpha vs X-ray or Gamma-ray radiation). Equivalent dose is the absorbed dose multiplied by a weighting factor • Effective dose: Accounts for varying sensitivity of tissues and organs to radiation. Effective dose is the sum of the equivalent doses to each tissue and organ exposed multiplied by tissue weighting factors, measured in seiverts (Sv = J/kg)
Ionizing Radiation • Radiation Dose • Range of effective doses for diagnostic imaging procedures ranges from 0.02 mSv for simple conventional X-rays to 200 mSv for certain angiography procedures • Much effort has been placed in determining the minimal dose amounts required to maintain image quality and diagnostic ability • Improving methods for X-ray detection and amplification, along with digital image manipulation hold promise for greater reductions in radiation exposure
Ionizing Radiation1 Dose in mGy or mSv Conventional X-rays 0.02-10 Conventional Complex X-rays 3-10 CT 5-15 Spiral CT 10-20 Angiography 10-200 Interventional 10-300 Nuclear imaging 3-14 Annual background radiation 2.4mSv 1. Health Risks From Exposure to Low Levels of Ionizing Radiation: BEIR VII Phase 2 2006.
Ionizing Radiation • Radiation Carcinogenesis • Believed most frequently to result from activation of proto-oncogenes or inactivation of tumor suppressor genes via aforementioned mechanisms • Most epidemiologic data is from high dose exposures, including atomic bomb survivors, occupational exposures, and therapeutic irradiation with extrapolation of risk for low dose exposure • A “stochastic effect”, linear model with no dose threshold is used for estimating risk of low dose exposures • Determining incidence of carcinogenesis is complicated by a long latency period, with some solid cancers manifesting 60 years after exposure • Increasing cancer incidence with earlier age at exposure
Ionizing Radiation • Radiation Carcinogenesis • Estimates for cancer risk: • Putman’s Textbook of Diagnostic Imaging: 10-5 risk of new cancer per mGy; or, 1 in 100,000 chance of new cancer per mGy • BEIR VII: 2270 total excess cancers and 1140 excess deaths per 100,000 persons exposed to 0.1Gy (100mGy); or, approximately 1 in 400 chance of new cancer and 1 in 800 chance of death if exposed to 100mGy
Ionizing Radiation1 Linear No Threshold High Dose Rate Linear Model With A Threshold Linear No Threshold Low Dose Rate Model Linear Quadratic Model • Linear no threshold model used for solid cancers • Linear quadratic better fits risk model for leukemia 1. Health Risks From Exposure to Low Levels of Ionizing Radiation: BEIR VII Phase 2 2006.
Ionizing Radiation1 Total 2270 1140 1. Health Risks From Exposure to Low Levels of Ionizing Radiation: BEIR VII Phase 2 2006.
Ionizing Radiation1 • It can be seen from this table, examining solid cancer incidence and mortality for men and women at different ages of exposure, that there is an increased incidence of solid cancer with earlier age at exposure 1. Health Risks From Exposure to Low Levels of Ionizing Radiation: BEIR VII Phase 2 2006.
Ionizing Radiation1 • This table illustrates the lifetime attributable risk for specific solid tumors among 105 persons after exposure to 0.1 Gy. Colon and lung cancer occur with greatest frequency in men compared with breast and lung cancer in women 1. Health Risks From Exposure to Low Levels of Ionizing Radiation: BEIR VII Phase 2 2006.
Ionizing Radiation1 • Unlike solid cancers, there does not appear to be a strong association between increased incidence of leukemia with earlier age at exposure 1. Health Risks From Exposure to Low Levels of Ionizing Radiation: BEIR VII Phase 2 2006.
Ionizing Radiation • Hereditary Effects of Radiation • Germline mutations • may lead to hereditary disorders in the progeny of irradiated persons • The risk is exceedingly low with diagnostic imaging and estimates are only indirectly available, rely heavily on mouse models, and pertain to continued low dose radiation exposure with risk calculated for dosing intervals of 1 Gy • Overall, the predicted risk per 1 Gy represents only 0.4-0.6% of baseline frequency of Mendelian, Chromosomal, and Multifactorial diseases in first generation progeny
Ionizing Radiation1 • This table shows there is an estimated increase of ~3000-4700 Mendelian, chromosomal, and multifactorial diseases within the first generation per Gy per million progeny with continued low dose exposure 1. Health Risks From Exposure to Low Levels of Ionizing Radiation: BEIR VII Phase 2 2006.
Ionizing Radiation • Hereditary Effects of Radiation • Infertility (occurring with gonadal irradiation) • Risk of permanent sterility exceedingly low with doses used for diagnostic imaging • Males: 0.15 Gy may cause oligospermia, 0.5 Gy may cause azoospermia and temporary sterility, 6 Gy or more may cause permanent sterility • Females: age dependent, may result in significant hormonal changes, 12 Gy in pre-pubertal and 2 Gy pre-menopausal may cause permanent sterility
Ionizing Radiation • Effects of Radiation on the Embryo and Fetus • Fetus particularly susceptible to effects of radiation due to rapid cellular growth with critical developmental stages • Effects dependent on dose and gestational age at exposure and include intra-uterine death, congenital malformations, growth retardation, mental retardation, and cancer • Association between x-ray exposure in utero and childhood malignancy exists, some reviews citing a 40% increase in relative risk following obstetric X-ray, with an excess absolute risk of about 6% per Gy • Recommended maximum monthly permissible dose to a fetus is 0.5 mSv • Dose of 0.1 Gy (100 mGy) between 10 days and 25 weeks gestation is often regarded as cutoff point above which therapeutic abortion is considered
Ionizing Radiation • Miscellaneous Factoids • Questions?
Contrast Media1 • Utilizing radiodense substances to help identify normal anatomic structures such as bowel wall and vasculature as well as pathologic conditions such as cancer and hemorrhage. • Types of contrast media: • Barium Sulfate agents • Water-Soluble agents • Oil-based agents • Paramagnetic (Gadolinium) agents (for use in MRI) • Micro-bubble based agents (for use in ultrasound) 1. From Daffner’s Clinical Radiology: The Essentials, Second Edition 1999
Contrast Media • Epidemiology of Adverse Reactions to Contrast: • Society of Radiology (n=150,000): • Overall incidence 5% • Severe reactions 1:1000-2000, death 1:13000-40000 • 2x risk with history of allergy • 3x risk with history of previous adverse reaction to contrast • Pre-testing and anti-histamine/steroid pre-treatment of no benefit • Japan/Australia Study (n=337,647) • Overall incidence with ionic contrast 12.7% • Incidence with low osmolar/non-ionic 3.1% • Serious reactions 0.22% (ionic) and 0.04% (low osmolar) • Recommend use of low osmolar agents when possible
Contrast Media • Characterization of adverse contrast reactions: • Typically mild and may affect CV, Respiratory, Dermatologic, GI, Nervous, and Urinary systems. • Mild (observation only): • Nausea, vomiting, sneezing, flushing, diaphoresis, warmth, headache • Intermediate (require treatment, eg benadryl/epinephrine): • Urticaria, angioneurotic edema, wheezing • Severe (emergent treatment, eg ABC’s, CPR): • Cardiovascular collapse, pulmonary edema, laryngeal edema, CNS depression, apnea, death
Contrast Media • Barium Sulfate: • Finely pulverized barium mixed with dispersing agents in water • Oral/rectal administration for outlining GI tract • Oral for obstruction proximal to ileocecal valve, rectal for obstruction distal to ileocecal valve: water absorbed by colon may thicken barium contrast and exacerbate colonic obstruction if given proximally (orally) • Contraindicated if perforation suspected: causes severe desmoplastic reaction outside of GI tract resulting in granuloma and adhesion formation
Contrast Media • Water-soluble: • Triiodobenzoic acid common chemical structure • Ionic: sodium or meglumine salts of diatrizoic or iothalamic acid • Ionic dimers: Linked triiodobenzoic molecules with only one sodium or meglumine cation • Non-ionic monomers: replaced sodium or meglumine cation with non-dissociable side-chain • CT, angiography, GI with suspected perforation, urography, arthrography, myelography, sinusography • Hypertonic (ionic>ionic dimer>non-ionic) with shift of fluid to intravascular or intraluminal compartments • Severity of side effects dependent on agent tonicity/viscocity, amount and rate of infusion, and patient susceptibility (eg dehydrated, renal or cardiac dysfunction)
Water-soluble agent adverse effects: Renal failure Bradycardia Decreased BP Decreased CO Bleeding from platelet aggregation abnormalities Chemical pneumonitis if aspirated Headache and Psych disturbance in myelography “Hypersensitivity” reaction Preventative measures Adequate hydration (eg intravenous fluid administration pre and post contrast) reduces risk of adverse reactions (eg renal failure) Use of N-acetyl cysteine can have reno-protective effects Low osmolality agents have significantly reduced incidence of serious adverse reactions but are more costly Oil-based or Barium agents may be used in cases of suspected esophagotracheal fistula to prevent chemical pneumonitis Contrast Media
MRI1 • Exposes the patient to an intense static magnetic field, a time variant magnetic field, and pulsed radiofrequency waves, and measures radiofrequency signals generated by nuclei with odd numbers of protons and neutrons (eg Hydrogen) that possess inherent magnetic dipoles to create tissue images • Some effects observed from large exposures include thermal effects, physiologic electric current generation, and ion conduction abnormalities, which may disrupt cell membranes, alter nerve conduction and CNS function, or cause electrophysiologic abnormalities such as EKG changes • Levels utilized currently are so low that significant effects are unlikely • Potential consequences from overheating or electric current generation does exist and has been observed for patients with pacemakers or other metallic implants or foreign bodies such as clips, prostheses, and metal shavings, with greatest concern for possible induction of cardiac arrhythmias • Anecdotes of headache, malaise, difficulty in concentration, sleep disturbance, EEG changes, metabolic/hematologic/immunologic changes have been reported with little substantiating evidence • MRI procedures often causes patient anxiety due to confinement and length of procedure, at times managed with benzodiazepine use--be cautious of psychological and pharmacologic reactions 1. From Putman’s Textbook of Diagnostic Imaging, Second Edition 1994.
Ultrasound1 • Acoustic wave form of energy that delineates structures of different acoustic impedance by detecting sound waves reflected from the interface of these structures • Carcinogenic, mutagenic, and teratogenic effects are zero or so low as to not be of concern in medical imaging • Damage can be thermal due to ultrasonic heating from wave absorption; and, non-thermal due to mechanical effects such as peak pressure areas, shock waves, and shear stresses at the interface of micro-cavitation bubbles • Experimentally produced damage in vitro and in vivo using animal models includes cell lysis, inactivation, altered growth, altered structure, modified synthetic pathways, and membrane instability, BUT mostly at intensity levels 10 to 1000 times greater than that used for diagnostic imaging 1. From Putman’s Textbook of Diagnostic Imaging, Second Edition 1994.
Summation • Imaging has a pivotal and expanding role in patient care • Risks of ionizing radiation and contrast media are relatively few and rare at the levels of exposure in diagnostic imaging, but must not be ignored • Remember first to do no harm—consider need for imaging and utilize the most appropriate studies to obtain desired information while minimizing risks • Appropriateness guidelines for imaging may be found at www.acr.org • The BEIR VII report on risks of low ionizing radiation may be viewed free online at www.nap.edu
References • Charles E Putman, Carl E Ravin. Textbook of Diagnostic Imaging, Second Edition. WB Saunders Company; Philadelphia 1994. • Eric J Hall, Amato J Giaccia. Radiobiology for the Radiologist, Sixth Edition. Lippincott Williams and Wilkins; New York 2006. • Health Risks From Exposure to Low Levels of Ionizing Radiation: BEIR VII Phase 2. The National Academies Press; New York 2006. (available online at www.nap.edu) • Luis Felipe Fajardo L-G, Morgan Berthrong, Robert E Anderson. Radiation Pathology. Oxford University Press; New York 2001. • Richard H Daffner. Clinical Radiology: The Essentials, Second Edition. Lippincott Williams and Wilkins; Baltimore 1999. • All picture images acquired from Google images and Wikipedia.