Download
1 / 1
10 likes | 98 Views
H-1892. Metabolic Syndrome and Cardiovascular Risk in Older HIV+ Patients: Data from the CORE50 Cohort K. REZAI , N. THOMAS-GOSSAIN, M. LEE, S. BADRI, O. M. ADEYEMI; CORE Ctr., Stroger Hosp. of Cook County, Chicago, IL. K. Rezai, MD 312-864-4552 Katayoun_rezai@rush.edu. RESULTS.

E N D
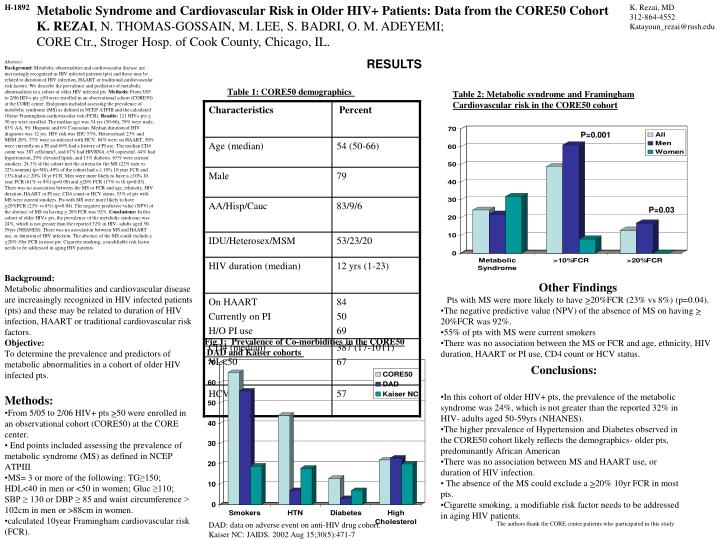
H-1892 Metabolic Syndrome and Cardiovascular Risk in Older HIV+ Patients: Data from the CORE50 Cohort K. REZAI, N. THOMAS-GOSSAIN, M. LEE, S. BADRI, O. M. ADEYEMI; CORE Ctr., Stroger Hosp. of Cook County, Chicago, IL. K. Rezai, MD 312-864-4552 Katayoun_rezai@rush.edu RESULTS Abstract:Background: Metabolic abnormalities and cardiovascular disease are increasingly recognized in HIV infected patients (pts) and these may be related to duration of HIV infection, HAART or traditional cardiovascular risk factors. We describe the prevalence and predictors of metabolic abnormalities in a cohort of older HIV infected pts. Methods: From 5/05 to 2/06 HIV+ pts >50 were enrolled in an observational cohort (CORE50) at the CORE center. End points included assessing the prevalence of metabolic syndrome (MS) as defined in NCEP ATPIII and the calculated 10year Framingham cardiovascular risk (FCR). Results: 121HIV+ pts > 50 yrs were enrolled. The median age was 54 yrs (50-66), 79% were male, 83% AA, 9% Hispanic and 6% Caucasian. Median duration of HIV diagnosis was 12 yrs. HIV risk was IDU 53%, Heterosexual 23% and MSM 20%. 57% were co-infected with HCV. 84% were on HAART, 50% were currently on a PI and 69% had a history of PI use. The median CD4 count was 387 cells/mm3, and 67% had HIVRNA <50 copies/ml. 44% had hypertension, 29% elevated lipids, and 13% diabetes. 65% were current smokers. 24.3% of the cohort met the criteria for the MS (22% men vs 32% women) (p=NS). 49% of the cohort had a ≥ 10% 10 year FCR and 13% had a ≥ 20% 10 yr FCR. Men were more likely to have a ≥10% 10 year FCR (61% vs 8%) (p=0.00) and >20% FCR (17% vs 0) (p=0.03). There was no association between the MS or FCR and age, ethnicity, HIV duration, HAART or PI use, CD4 count or HCV status. 55% of pts with MS were current smokers. Pts with MS were more likely to have >20%FCR (23% vs 8%) (p=0.04). The negative predictive value (NPV) of the absence of MS on having > 20%FCR was 92%. Conclusions: In this cohort of older HIV+ pts, the prevalence of the metabolic syndrome was 24%, which is not greater than the reported 32% in HIV- adults aged 50-59yrs (NHANES). There was no association between MS and HAART use, or duration of HIV infection. The absence of the MS could exclude a >20% 10yr FCR in most pts. Cigarette smoking, a modifiable risk factor needs to be addressed in aging HIV patients. Table 1: CORE50 demographics Table 2: Metabolic syndrome and Framingham Cardiovascular risk in the CORE50 cohort P=0.001 P=0.03 Background: Metabolic abnormalities and cardiovascular disease are increasingly recognized in HIV infected patients (pts) and these may be related to duration of HIV infection, HAART or traditional cardiovascular risk factors. Objective: To determine the prevalence and predictors of metabolic abnormalities in a cohort of older HIV infected pts. • Other Findings • Pts with MS were more likely to have >20%FCR (23% vs 8%) (p=0.04). • The negative predictive value (NPV) of the absence of MS on having > 20%FCR was 92%. • 55% of pts with MS were current smokers • There was no association between the MS or FCR and age, ethnicity, HIV duration, HAART or PI use, CD4 count or HCV status. Fig 1: Prevalence of Co-morbidities in the CORE50 DAD and Kaiser cohorts • Conclusions: • In this cohort of older HIV+ pts, the prevalence of the metabolic syndrome was 24%, which is not greater than the reported 32% in HIV- adults aged 50-59yrs (NHANES). • The higher prevalence of Hypertension and Diabetes observed in the CORE50 cohort likely reflects the demographics- older pts, predominantly African American • There was no association between MS and HAART use, or duration of HIV infection. • The absence of the MS could exclude a >20% 10yr FCR in most pts. • Cigarette smoking, a modifiable risk factor needs to be addressed in aging HIV patients. • Methods: • From 5/05 to 2/06 HIV+ pts >50 were enrolled in an observational cohort (CORE50) at the CORE center. • End points included assessing the prevalence of metabolic syndrome (MS) as defined in NCEP ATPIII • MS= 3 or more of the following: TG≥150; HDL<40 in men or <50 in women; Gluc ≥110; SBP ≥ 130 or DBP ≥ 85 and waist circumference > 102cm in men or >88cm in women. • calculated 10year Framingham cardiovascular risk (FCR). DAD: data on adverse event on anti-HIV drug cohort. Kaiser NC: JAIDS. 2002 Aug 15;30(5):471-7 The authors thank the CORE center patients who participated in this study