Download
1 / 12
120 likes | 284 Views
Amiodarone Use in Cardiac Surgical Resuscitation. Jeffrey R. Balser, M.D., Ph.D. Associate Professor, Anesthesiology and Pharmacology Associate Dean, Physician Scientist Development Vanderbilt University School of Medicine Nashville, TN 37232. Ventricular Arrhythmias. Arrhythmia.

E N D
Amiodarone Use in Cardiac Surgical Resuscitation Jeffrey R. Balser, M.D., Ph.D. Associate Professor, Anesthesiology and Pharmacology Associate Dean, Physician Scientist Development Vanderbilt University School of Medicine Nashville, TN 37232
Ventricular Arrhythmias Arrhythmia Common Substrates normal ventricle, periop • PVCs, nonsustained VT prior MI, structural disease • Sustained monomorphic VT • Polymorphic VT with normal QT acute ischemia, infarction, idiopathic cardiomyopathy Ventricular fibrillation • Polymorphic VT with congenital, prior drugs, low K, Mg, bradycardia prolonged QT interval (torsade de pointes)
Most common sustained VT/VF in cardiac surgery • Normal QT Polymorphic VT (ischemia, hypothermia, infarction,) • Ventricular Fibrillation (VF) - Little data on pharmacologic therapy for VT/VF in surgical patients… however, there are recent data in nonsurgical patients
IV Amiodarone in ICU patients • Recurrent VT/VF refractory to lidocaine, procainamide, and bretylium: • 40% arrhythmia-free at 24 hrs JACC 27:67, 1996 • After lidocaine and procainamide failure • efficacy: bretylium = amiodarone • side effects: bretylium > amiodarone Hypotension: 33% vs. 21% CHF: 5% vs. 0% Circ 92:3255, 1995
IV Amiodarone in Cardiac Arrest 504 victims of out-of-hospital cardiac arrest in Seattle • IV amiodarone (300 mg) or vehicle control • administered by emergency personnel following • 3 defibrillation attempts and 1 mg of epinephrine • while CPR continued. • The likelihood of being resuscitated and being admitted to the hospital was 44% in the treatment group vs. 34% in the placebo arm (p = 0.03) Kudenchuk et al., N Engl J Med. 1999;341:871-8
Recent Recommendations for VT/VF Management in Cardiac Arrest Airway, Breathing, etc.. Defibrillatory Shocks If refractory: consider antiarrhythmic drugs amiodarone (IIb), lidocaine (Indeterminate), magnesium (IIb if hypomagnesemic state) procainamide (IIb for intermittent/recurrent VF/VT) Circulation 2000 (Aug 22), 102:I-147
Evidence-based recommendations: Terminology IIb (Amiodarone, Procainamide) • Consensus review of evidence by experts in the field suggest the intervention is “Fair to Good” • Considered within “standard of care”: reasonably prudent physicians can use. • Considered optional or alternative interventions by majority of experts (versus an intervention of choice for IIa recommendation) Circulation 2000 (Aug 22), 102:I-147
Evidence-based Recommendations: shock-refractory VT/VF Lidocaine: new recommendation is “Indeterminate” Lidocaine has not been shown to be effective in treating human cardiac arrest during shock-resistant VF Circulation 2000 (Aug 22), 102:I-149
Unique Features of IV Amiodarone • No known value to combine with other agents - usually discontinue lidocaine, procainamide, and other antiarrhythmic agents when using IV amiodarone • Loading is empiric - 150 mg IV (rate as hemodynamically tolerated) - 2-4 loading doses are often needed - more are not unheard of….
IV Amio in Electrical Storm Typical Scenario load IV amio (150 mg/5-10 min) Shock VF VF! (CPR) VF recurs (10 sec) sinus rhythm 6 hrs: amio to 0.5 mg/min (30 sec) sinus rhythm Shocks VF recurs sinus rhythm (for now)... reload IV amio shock VF Shock VF reload IV amio (no agent change)! sinus rhythm lasting 5-10 min 1 min later: VF recurs start amio infusion: 1 mg/min (6 hrs)
Features of IV Amiodarone Use • Rarely chemically converts VF -- maintains SR after defibrillatory shocks - load, shock, SR, VF, load, shock, SR…. Sign of drug “response” may be gradual lengthening of the interval of SR between episodes of VF • Amiodarone and its solvent are both vasodilators - pressors may be needed to support BP during amiodarone loading (especially in SR)
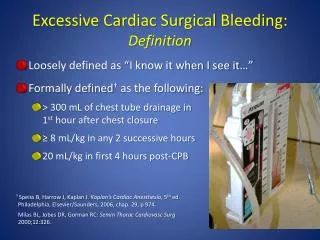
Summary: VT/VF Pharmacologic Strategies in Cardiac Surgery • Nonsustained VT: Usually does not require drug therapy • Sustained VT/VF: • - Drug-induced Long QT, Torsades de Pointes: • Defibrillation, then K+, Mg2+, pacing - Other VT/VF: No controlled trials in surgical patients - data in other settings (ICU, out-of-hospital) support the use of IV amiodarone in preference to lidocaine