Download
1 / 52
520 likes | 610 Views
The Body Sense and Movement Chapter 11. The Body Senses. We get information about our body from the somatosensory system and the vestibular system. The somatosenses include: the skin senses, which tell us about conditions at the surface of our body.

E N D
The Body Senses • We get information about our body from the somatosensory system and the vestibular system. • The somatosenses include: • the skin senses, which tell us about conditions at the surface of our body. • proprioception, which provides information about limb and body position and movement. • the interoceptive system, concerned with sensations in our internal organs. • The vestibular system informs the brain about head position and movement and helps us maintain balance.
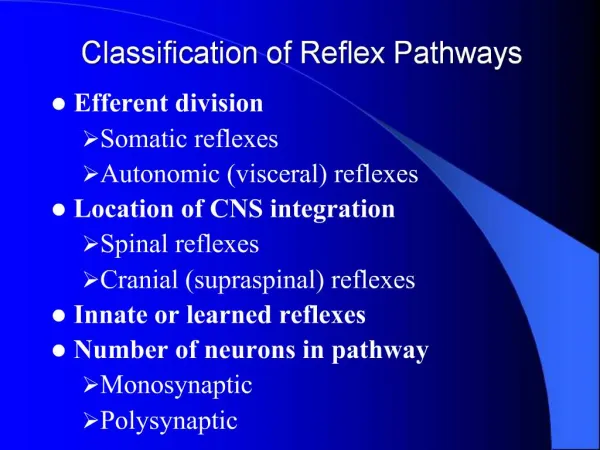
The Body Senses • The skin senses are touch, warmth, cold, and pain. • Itch was thought to be a variant of pain, but may be a fifth sense; it can be eliminated without affecting pain sensitivity. • There are two general types of receptors. • Free nerve endings • are processes at the ends of neurons; • detect warmth, cold, and pain. • All the other receptors areencapsulated receptors, more complex structures enclosed in a membrane. • Their role is to detect touch.
The Body Senses • Receptors for Touch • In the superficial layers of the skin • the receptors areMeissner’s corpuscles and Merkel’s discs; • they detect texture and fine detail of objects. • In the deeper layers of the skin • the receptors arePacinian corpuscles and Ruffini endings; • they detect stretching of the skin and contribute to our perception of grasped objects. ◊
The Body Senses • The density of skin receptors varies throughout the body; sensitivity varies with the density. • The lips and the fingertips are the most sensitive. • Upper arms and calves of the legs are least sensitive. ◊
The Body Senses • Free nerve endings detect temperature and pain, but each has distinctly different receptors. • Detection of temperature involves thetransient receptor potential or TRPfamily of protein ion channels. • Pain detection requires several receptors, depending on the type of pain. • Mechanical pain: the receptors have not yet been identified. • Chemical pain: the TRPA1 receptor accounts for the pain caused by tear gas, tobacco smoke, and some foods, such as garlic and wasabi. ◊
The Body Senses • Thermal pain: two TRP receptors respond to painful heat. • Best known is the TRPV1 heat pain receptor, which responds to capsaicin, found in chili peppers. Capsaicin alleviates pain in joints by fatiguing the receptors. • Menthol creams are useful for treating muscle pain and skin irritations, because they stimulate the TRPM8 coolness receptor. ◊
The Body Senses • The vestibular sense helps us maintain balance, and it provides information about head position and movement. • The vestibular organs, found in the inner ear, are the semicircular canals, the utricle, and the saccule. • The vestibular system sends projections to the cerebellum and the brain stem. • There is also a pathway to a cortical area called the parieto-insular-vestibular cortex, which is probably the site of movement induced dizziness and nausea. ◊
The Semicircular CanalsFigure 11.2 a & b • The semicircular canals respond to movement of the head (and, therefore, of the body). • Hair cells are imbedded in thecupula, a jelly-like substance found at the base of each canal. This produces depolarization or hyperpolarization, depending on the direction of movement. • Acceleration causes fluid in the canals to displace the cupula.
The Utricle and SacculeFigure 11.2c • The utricule and saccule monitor head position in relation to gravity. • The hair cells are embedded in a gelatinous mass, so they are activated when the head tilts. • A horizontal patch of hair cells and a vertical patch provide tilt information in two planes. ◊
The Body Senses • The body is divided into segments called dermatomes, each served by a spinal nerve. • Body sense information enters the spinal cord (via spinal nerves) or the brain (via cranial nerves) and travels to the thalamus. • From there the body sense neurons go to the somatosensory cortex (located in the parietal lobes just behind the primary motor cortex and the central sulcus). • Most of the neurons cross from one side of the body to the other side of the brain, so the touch of an object held in the right hand is registered mostly in the left hemisphere. ◊
The Body Senses • The somatosensory system shares a number of features with other sensory systems: • Somatosensory processing is hierarchical: • The somatosensory cortex contains a map of the body. • The area devoted to a part of the body corresponds to the sensitivity of the body part. Information travels from the primary somatosensory cortex to the secondary somatosensory and to cortex parietal and temporal lobes
The Body Senses • Some cortical cells have complex receptive fields on the skin, with excitatory centers and inhibitory surrounds. • These cells are feature detectors for orientation, direction of movement, shape, and texture.
The Body Senses • The secondary somatosensory cortex receives input from the left and the right primary somatosensory cortices, so it combines information from both sides of the body. • Neurons in this area are particularly responsive to stimuli that have acquired meaning, for instance, by association with reward. • The secondary somatosensory cortex connects to the part of the temporal lobe that includes the hippocampus, which is important in learning, • so it may serve to determine whether a stimulus is committed to memory.
The Body Senses • The posterior parietal cortex is an association area that brings together the body senses, vision, and audition. • Here the brain determines the body’s orientation in space, the location of the limbs, and the location in space of objects. • Cells are specialized for functions such as posture and reaching and grasping. • Damage to this area can produce neglect. • Other anomalies associated with the area are body integrity identity disorder and out-of-body experiences. ◊
The Body Senses • Pain begins when certain free nerve endings are stimulated by intense pressure or temperature, by damage to tissue, or by various chemicals. • This intense stimulation may trigger inflammation by causing cells to release a wide array of signaling molecules, referred to as the “inflammatory soup”. • Pain information travels to the spinal cord by two routes. • Large, myelinated A-delta fibers transmit sharp pain right after an injury has occurred. • Small, unmyelinated fibers respond more slowly, and are responsible for the delayed, longer-lasting dull pain. ◊
The Body Senses • The spinal cord releases glutamate and, during intense pain stimulation, substance P. • Pain information travels via the thalamus to the somatosensory cortex and to areas that process emotional aspects of pain. ◊
The Body Senses • Treating Pain • Local anesthetics block sodium channels in the pain neurons and reduce their ability to fire. • General anesthetics act in the CNS. • Common pain medications include aspirin, ibuprofen, and acetaminophen (Tylenol). • Aspirin and ibuprofen reduce inflammation by suppressing prostaglandin synthesis. • Morphine and similar opiate drugs are effective painkillers, but they show rapid tolerance and are addictive. • Alternative medications include the MDAN series, as well as the drug Tanezumab, an antibody for nerve growth factor.
The Body Senses • Internal Mechanisms of Pain Relief • Endorphinsfunction both as neurotransmitters and as hormones, and act at opiate receptors in many parts of the nervous system. • Pain causes the release of endorphins, but only under certain conditions. • Endorphin release and pain reduction occur during: • inescapable shock; • physical stress; • acupuncture; • vaginal stimulation (most likely linked to childbirth); • placebo administration.
The Body Senses • Pain relief that involves endorphins is reversed by naloxone, an opiate antagonist. • Some stimulus-induced pain relief is not reversed by naloxone, and is due to other means of internal analgesia. • Pain relieving stimulus conditions that do not depend on endorphins include hypnosis and acupuncture near the pain site. • A circuit involved in internal pain relief was proposed by Melzack and Wall in their gate control theory. • In their theory, pressure triggers an inhibitory message that closes a neural “gate” in the pain pathway. ◊
The Descending Pain Inhibition CircuitFigure 11.8 • Pain causes the release of endorphins from the periaqueductal gray in the brain stem. • This inhibits the release of substance P, closing the pain ”gate” in the spinal cord. • The endorphin circuit is activated by the cingulate cortex during placebo administration, and by the amygdala during fear.
The Body Senses • Pain’s Extremes • People withcongenital insensitivity to painmay be unaware of injuries and may be inadequately motivated to avoid injury. • A mutation in the SCN9A gene produces nonfunctional versions of a sodium channel, disabling pain neurons. • A mutation in the gene for nerve growth factor (NGFB) reduces the number of neurons. • A third possible cause is high levels of endogenous opioids. ◊
The Body Senses • Chronic painis pain that persists after healing has occurred. • Nociceptive pain involves activation of the pain receptors. • Neuropathic pain is caused by damage to the CNS or PNS. • Genes that reduce pain thresholds (including a different allele of the SCN9A gene) increase susceptibility to chronic pain. • Several changes occur in the PNS and in the CNS, including loss of gray matter equivalent to aging 10-20 years.
The Body Senses • Phantom Pain • 80% to 90% of amputees experience phantom in the missing limb. • In these individuals neurons from other body areas invade the area that normally receives input from the missing limb. Figure 11.10
The Body Senses • Therapies that relieve phantom pain prevent or reverse this reorganization. • Using a functional prosthesis or the mirror box illusion reverses the cortical reorganization and provides pain relief. • One interpretation of the mirror box effect: • It activates mirror neurons in the area that once served the missing limb. • This activity is interpreted as real touch and movement, and this stimulates reorganization. ◊
Movement • The Muscles • Skeletal muscles move the body and limbs. • They are also called striated muscles because of their striped appearance. • Smooth muscles produce the movements of the internal organs. • Cardiac muscles are the muscles that make up the heart. ◊
Movement • Like other tissues of the body, a muscle is made up of many individual cells, or muscle fibers. • A muscle fiber is made up of myosin and actin filaments. • When a motor neuron releases acetylcholine the muscle fiber is depolarized, which opens calcium channels. • The myosin filaments “climb” along the actin filaments, which shortens and contracts the muscle. ◊
Movement • Antagonistic muscles are muscles that produce opposite movements at a joint. • For example, the bicep muscle flexes the arm, and the triceps extends it. • These muscles work together to produce smooth movements and to maintain a position, as in standing. ◊
Movement • Muscle stretch receptors are called muscle spindles. • They initiate reflexes that oppose activity in the antagonistic partner. • This helps in maintaining posture and responding to a sudden load. ◊ Figure 11.13
Movement • Golgi tendon organs detect tension in a muscle. • They prevent muscles from stretching to the point of damage. • Central pattern generators are neuronal networks that produce rhythmic patterns of motor activity. • These aid in walking, swimming, flying, and breathing. • They may be located in the spinal cord or in the brain. • They can be elicited in people with spinal cord injury to produce rhythmic stepping movements. ◊
Movement • The Brain and Movement • The primary and two secondary motor cortices contain a map of the body; the amount of cortical area corresponds to the fineness of movement in that part of the body. • Theprefrontal cortex • integrates auditory and visual information with information from the posterior parietal cortex • and holds the information in memory • while selecting the appropriate movement and its target. ◊
Movement • The premotor cortex begins programming a movement by combining information from the prefrontal cortex and the posterior parietal cortex. • Its output flows to the supplementary motor area, which assembles complex sequences of movements. • The primary motor cortex is responsible for the execution of voluntary movements. • Its cells fire most during the movement instead of prior to it. • Individual cells are not allocated to specific movements, but contribute to a range of related behaviors.
Movement • The primary motor cortex orchestrates the activity of these cells into a useful movement and contributes to its force and direction. • The primary motor cortex puts a sequence of behaviors together with help from the secondary motor cortex, the somatosensory cortex, and the posterior parietal areas. • The somatosensory cortex and posterior parietal areas provide feedback for refining movements “on the fly”. ◊
Movement • The basal ganglia • receive information from the primary and secondary motor areas and the somatosensory cortex; • and smooth movements, apparently by sending excitatory and inhibitory outputs through the thalamus back to motor areas. • They apparently are also involved in learning movement sequences that can be performed as a unit. ◊
Movement • The cerebellum • receives information from the motor cortex about an intended movement and determines the order and timing of muscular contractions; • uses information from the vestibular system to • maintain posture and balance, • refine movements, • and control eye movements that compensate for head movements. • plays a role in learning skilled movements; • is involved in nonmotor tasks.
Movement • Parkinson’s Disease • Symptoms are motor tremors, rigidity, loss of balance and coordination, and difficulty in moving, especially in initiating movements. • The symptoms are caused by deterioration of the substantianigra, which sends dopamine-releasing axons to the striatum. • The striatum is composed of the basal ganglia’s caudate nucleus and putamen and the nucleus accumbens. • So, dopamine is lost in an important motor circuit. ◊
Movement • Genes appear to be involved in less than 10% of Parkinson’s cases, those occurring before age 51. • The genes that have been implicated are involved in: • development and programmed death of dopamine-producing neurons; • development of Lewy bodies, protein clumps that form in neurons; • diminished ability to metabolize environmental toxins. ◊
Lewy Bodies in Parkinson’s DiseaseFigure 11.20 The two dark spots are Lewy bodies
Movement • Environmental Influences in Parkinson’s Disease • Parkinson’s may be caused by subtle brain injury and by toxins such as carbon monoxide, herbicides, and pesticides • Caffeine blocks adenosine receptors, which increases dopamine and acetylcholine release, and reduces risk by 80%. • Smoking may prevent accumulation of neurotoxins, but at greater cost than benefit. ◊
Movement • Huntington’s Disease • Degenerative disorder of the motor system involving cell loss in the striatum and cortex. • Motor symptoms (writhing, grimacing) are due to degeneration of neurons in the striatum. • Other symptoms include • cognitive impairment, • depression, • and personality changes, • which are likely caused by the cortical neuron deficits.
Movement • Huntington’s disease is caused by a dominant mutation in the huntingtingene. • The gene ordinarily has 10 to 34 repetitions of the bases cytosine, adenine, and guanine. • The more repetitions the person has beyond 37, the earlier in life the individual will succumb. • Neuron loss is probably due to accumulation of the gene’s protein. • The only drug approved for Huntington’s reduces excess dopamine. • A promising anti-glutamate drug may prevent cell death from overstimulation.
A Huntington’s Disease BrainFigure 11.24 Arrows point to the caudate nucleus in a normal brain (left) and a diseased brain (right).
Movement • Myasthenia gravis • This is a disorder of muscular weakness caused by reduced numbers or sensitivity of acetylcholine receptors. • Acetylcholinesterase inhibitors increase acetylcholine at the neuromuscular junction and give temporary relief. Figure 11.23: A patient before and after acetylcholinesterase inhibitor
Movement • Removal of the thymus has become a standard therapy • For myesthenia gravis. • This decreases the number of lymphocytes that produce antibodies. • Thymectomy completely eliminates symptoms in almost 80% of patients. • Success of this treatment supports the conclusion that it is an autoimmune disease. ◊
Movement • Multiple sclerosis is a motor disorder with many varied symptoms, caused by deterioration of myelin (demyelination) and neuron loss in the CNS. • Demyelination causes slowing or elimination of neural impulses, reducing the speed and strength of movements. • Demyelinated neurons die, leaving hardened scar tissue. ◊