Download
1 / 25
250 likes | 391 Views
Remote SFA Endarterectomy How I Do It. David Rosenthal, MD. SFA (> 20 cm). PTA Stent LA Atherectomy. “REMOTE” SFA ENDARTERECTOMY. Performed through small incision “Debulked” arterial plaque Endovascular stent Durable SFA procedure?. Vollmar Stripper. Martin Dissector.

E N D
Remote SFA Endarterectomy How I Do It David Rosenthal, MD
SFA (> 20 cm) PTA Stent LA Atherectomy
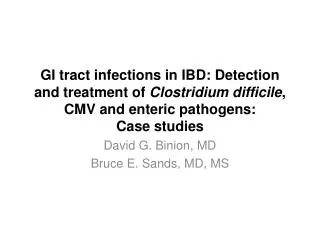
“REMOTE” SFA ENDARTERECTOMY • Performed through small incision • “Debulked” arterial plaque • Endovascular stent • Durable SFA procedure?
Vollmar Stripper Martin Dissector Fogarty Endohelix MollRing Cutter
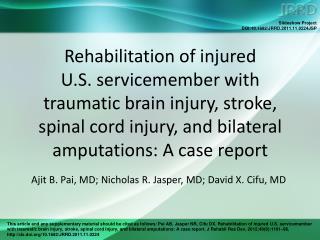
“TACK” DISTAL PLAQUE BALLOON STENT ANGIOPLASTY
Non-flexible Stent aSpire Stent aSpire Stent
PURPOSE Retrospective, multicenter study was to examine the medium-term results of remote superficial femoral artery endarterectomy (RSFAE) and distal aSpire stenting.
STUDY GROUP (n=235) • Indications for procedure: Claudication in 188 Limb Salvage in 47 • All patients underwent serial duplex color-flow ultrasound scanning during follow-up. RISK FACTORS Percent (%)
RESULTS • One death • Wound complications in 2% • Mean length of endarterectomized SFA=28.2cm • Mean hospital LOS 1.3 days
Nine over course SFA • Eight at adductor canal • Seven at distal stent Intimal hyperplasia ? . RESTENOSIS (n=24) = 9%
LONG SEGMENT SFA NOTSUCCESSFULLY TREATED Small caliber artery Disease long & diffuse Tortuous Low Flow Compression forces
DEBULKING SFA • Increase diameter • Reduce recoil & remodeling • Preserving collaterals • Durable procedure
CONCLUSION CONCLUSION If RSFAE and distal aSpire stenting long-term patency rates similar to AKFP, it may prove to be minimally invasive durable adjunct for treatment of SFA occlusive disease.