Download
1 / 33
870 likes | 2.5k Views
CYSTINURIA. By DR Jameel Tariq Miro. Cystinuria is an autosomal recessive defect in reabsorptive transport of cystine and the dibasic amino acids ornithine, arginine, and lysine from the luminal fluid of the renal proximal tubule and small intestine. Pathophysiology.

E N D
CYSTINURIA By DR Jameel Tariq Miro
Cystinuria is an autosomal recessive defect in reabsorptive transport of cystine and the dibasic amino acids ornithine, arginine, and lysine from the luminal fluid of the renal proximal tubule and small intestine.
Pathophysiology Renal transport of cystine • Amino acids filtered undergo nearly complete reabsorption by proximal tubular cells. • Only 0.4% of the filtered cystine appears in the urine. • . At least 2 transport systems are responsible for cystine reabsorption, as follows: - High-affinity system: This system is affected in persons with cystinuria. Mediates uptake of 10% of L-cystine and the dibasic amino acids at the third segment (S3) of the proximal tubule. - Low-affinity system: This system is present in the S1-S2 part of the proximal tubule and is responsible for 90% of L-cystine reabsorption. .
Intestinal transport of cystine • The high-affinity transporter is present in the apical brush-border membrane of the jejunum and is responsible for absorption of cystine and dibasic amino acids. • Most patients with cystinuria have impaired absorption of cystine; however, cystine deficiency is not clinically significant .
Normally, cystine and the other dibasic amino acids (ie, ornithine, lysine, arginine) are filtered at the glomerulus and reabsorbed in the proximal convoluted tubule . Defects in this channel cause elevated levels of dibasic amino acid secretion in the urine. Whereas ornithine, lysine, and arginine are completely soluble, cystine is relatively insoluble at physiologic urine pH levels of 5-7 . At a urine pH level of 7.8 and 8, the respective solubility of cystine is nearly doubled and tripled
The solubility of cystine is pH-dependent -Approximately 250 mg/L (1 mmol/L) up to a pH 7, -Increases up to 500 mg/L (2 mmol/L) or more above a pH 7.5 - Varies depending on the particular type of electrolyte present - Highest is accomplished in the presence of calcium chloride, followed by magnesium and sodium chloride. -Also affected by urinary macromolecules. The presence of colloid in normal urine has been shown to increase cystine solubility; however, the mechanism of this action is not clear. .
Risk factors for cystine crystallization include (1) low pH level (2) reduced ion strength, (3) the presence of cystine crystals, and (4) low levels of urinary macromolecules. Two thirds of persons with cystinuria who form stones make pure cystine calculi, One third have a mixture of cystine and calcium oxalate calculi. Hypocitraturia, hypercalciuria, and hyperuricosuria are also frequently associated with cystinuria. Pure cystine calculi are among the hardest on Dretler's stone fragility index.
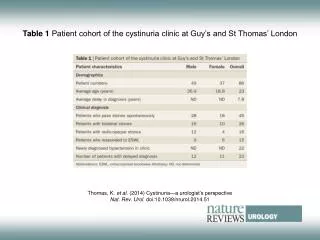
In healthy individuals, the upper limit for cystine excretion is 20 mg/g of creatinine (<10 µmol/mmol of creatinine). Homozygotes excrete more than 400 mg/d (1.7 mmol/d), and cystine excretion in homozygous patients is usually 600-1400 mg/d (2.5-5.8 mmol/d). Heterozygotes with type I and III cystinuria excrete less than 200 mg/d (0.8 mmol/d) and do not form stones. Type II heterozygotes excrete up to 200-400 mg/d, but these patients may form stones. The incidence of stone formation increases when urinary cystine concentration exceeds 700 µmol/L (170 mg/L).
Frequency United States Cystine accounts for 1% of adult and 6-8% of pediatric urinary calculi. The prevalence of heterozygosity is approximately 1 case per 20-200 persons. Homozygous cystinuria affects 1 person per 15,000 population. International Worldwide, the overall prevalence is 1 person per 7000 population. 1 case in 1900 in Spain, to 1 case in 100,000 in Sweden. Race Cystinuria is more common in white persons. Sex Incidence is equal between the sexes, but men are more severely affected. Age The peak age of first renal calculus is 22 years, up to 22% develop calculi in childhood.
presentation Presentation is similar to that of other types of renal calculi and includes renal colic, chronic urinary tract infections in a young person with a family history of kidney stones, passage of stones or gravel, hematuria, and dysuria. Uncommon presentations include chronic backache, and urinary tract infection. 25% of symptomatic patients report their first stone in the first decade of life, and another 30-40% have their first experience as teenagers. 20-40% of the stones in persons with cystinuria are mixed Homozygous cystinuria is characterized by lifelong, recurrent urolithiasis that is difficult to manage, either surgically or medically. . Seventy-five percent of these patients present with bilateral calculi. Recurrence rates after surgical intervention approach 45% at 3 months without medical management. The recurrence rate with medical management improves to approximately 25% at 3 years after surgery
Lab Studies 1-Urinalysis Cystine is one of the sulfur-containing amino acids; therefore, the urine may have the characteristic odor of rotten eggs. may show typical hexagonal or benzene crystals, which are essentially pathognomonic of cystinuria. Microscopic crystalluria is present in 26-83% of patients. Disappearance of cystine crystals in the first morning urine is a good index of treatment efficacy. . Measurement of urine cystine capacity: a measure of the ability of urine either to take up additional cystine from a preformed solid phase or to give it up to the solid phase . Cystine capacity can be used to monitor the response to the drug therapy and can help the clinician to prescribe minimal effective dose Cystine crystal volume from microscopic analysis of early-morning urine to predict stone recurrence.
2-Sodium cyanide–nitroprusside test a rapid, simple, and qualitative determination of cystine concentrations. Cyanide converts cystine to cysteine. Nitroprusside then binds, causing a purple hue in 2-10 minutes. The test detects cystine levels of higher than 75 mg/g of creatinine. False-positive test results occur in some individuals with homocystinuria or acetonuria and in people taking sulfa drugs, ampicillin, or N-acetylcysteine.. For individuals with positive cyanide-nitroprusside test findings, perform ion-exchange chromatographic quantitative analysis of a 24-hour collected urine sample. • The normal excretion rate is 40-80 mg/d (0.166-0.333 mmol/d). • Heterozygotes excrete 200-400 mg/d (0.8-1.7 mmol/d). • Homozygotes always excrete 600-1400 mg/d (2.5-5.8 mmol/d).
3- Twenty-four–hour urine collection for other metabolic abnormalities Results indicate the presence of hypercalciuria, hypocitraturia, and hyperuricosuria. Results may help define a subgroup of patients at risk for failure of medical therapy due to the formation of noncystine or mixed calculi. 4- Routine monitoring of renal function: Patients can self-monitor urine pH with Nitrazine paper. 5- Proton nuclear magnetic resonance spectroscopy of urine very powerful technique that allows multicomponent analysis useful in both diagnosis and follow-up. the relevant amino acids can be detected in the urine of patients with cystinuria. The most abundant amino acid in these patients is lysine (>5 mmol), whose typical signals become very high. Cystine, arginine, and ornithine are usually detectable, although pathologic concentrations are lower (<2 mmol). .
Imaging Studies Plain radiographs Cystine stones have a homogeneous or ground-glass appearance on radiographs . Although radiopaque, they are often less dense than calcium-containing stones. Intravenous pyelograms are essential for defining calyceal anatomy prior to extracorporeal shockwave lithotripsy (ESWL). Helical CT scan without intravenous contrast Helical CT scans are ideal for patients with contrast allergy or renal insufficiency. Renal ultrasonography This study is more economical than CT scan for monitoring the growth of renal calculi The lack of radiation exposure makes this test ideal for children and patients with frequent recurrences, who would otherwise accumulate relatively large radiation doses over a lifetime.
Management • Management algorithm • for a patient with cystinuria who does not have a stone, first-line therapy in most cases is a conservative approach, -large-volume fluid intake (urine output >2.5 L/d), -urine pH monitoring (urine pH level of 7.5 and <8), - -dietary restrictions, and urinary alkalization with potassium citrate. • If this standard therapy fails to achieve the urinary cystine concentration of 300 mg/L, then medical therapy with D-penicillamine, alpha-MPG, or captopril must be added. • Treat patients with stone disease according to the location of the stone. The expertise of a urologist and a radiologist is important for decision-making processes, and stone site and size also influence further management
Medical Hydration the oldest and most effective cystine stone–prevention techniques is hyperdiuresis to decrease urinary cystine concentration. that hydration alone could prevent stone recurrence in up to a third of patients. The goals of hydration therapy are urine volumes in excess of 3 L/d. This goal may require ingesting 4-4.5 L of water per day. Patients should drink 240 mL of water every hour during the day and 480 mL before retiring and at least once during the night. Patients should monitor the specific gravity of their urine using Nitrazine dipsticks, with a goal of achieving a value less than 1.010.
Alkalinization • Alkaline urine can prevent the precipitation of cystine calculi and can even aid in dissolution. Urine pH level must be more than 7.5 for stone dissolution to occur. • Paradoxically, a urine pH level of more than 7.5 can cause a predisposition to the formation of calcium phosphate calculi, so urine must be monitored with dipsticks to maintain a pH level of 7-7.5 for stone prevention. • Sodium bicarbonate was used in the past but is no longer recommended as a first-line agent. The sodium ion may actually increase the amount of cystine excreted. • Potassium citrate is the first-line alkalinizing drug. • With any alkalinization therapy, monitoring of urinary pH is essential.
Chelating agents Cystine-binding and cystine-reducing agents share the ability to dissociate the cystine molecule into disulfide moieties with much higher solubilities than the parent molecule. These drugs are thiol derivatives. The treatment goal is excretion of less than 200 mg/d of urinary cystine, and this must be monitored yearly. Start these agents when hydration, dietary, and alkalinization therapies fail. Cystine-binding agents can dissolve cystine calculi, but usually takes many months to years. They are best suited for stone prevention after surgical debulking of the stone burden, and they possibly help soften cystine stones in preparation for ESWL.
Penicillamine Penicillamine is a first-generation chelating agent that combines with cystine to form a soluble disulfide complex (50 times more soluble than cystine), thus preventing stone formation and possibly even dissolving existing cystine stones. The effect of the drug is dose-dependent. Adverse reactions (pproximately 50%) ; therefore, routine use is limited. include rash, arthralgia, leukopenia, gastrointestinal intolerance, and nephritic syndrome. Long-term therapy may lead to vitamin B-6 (pyridoxine) deficiency; thus, vitamin B-6 supplementation (50 mg/d) is needed.
Alpha-mercaptopropionylglycine This second-generation chelating agent Alpha-MPG has a 30% higher dissolution capacity for cystine than penicillamine. The drug is not excreted in the urine, so the cyanide-nitroprusside test is an effective qualitative screening method for monitoring the control of cystinuria. A positive test result indicates the need for an increased dosage. The main advantage of thiol is its lower toxicity profile.
Captopril Captopril can be used to treat patients whose conditions fail to respond to standard treatment and to treat patients with cystinuria who are hypertensive. Bucillamine a third-generation chelating agent available only in Japan and South Korea. showed a low toxicity profile; therefore, it is probably well tolerated by patients with cystinuria.
Diet Cystine is formed during the metabolism of methionine; therefore, a diet low in methionine is effective. dietary methionine must be reduced to 1 g/d. (0.8 g protein/kg body weight/d) is recommended. Dietary restriction of methionine found in animal proteins such as milk, eggs, cheese, and fish may be helpful Low-sodium diet Glutamine Increase dietary fiber intake
Surgical Care • Indications • large calculi that are unlikely to dissolve • obstructing or otherwise symptomatic calculi. • The ultimate goal of surgery is to make the patient free of stones. While the risk of recurrence is unchanged, the time to recurrence is significantly lengthened.
Surgical options (1) ESWL, (2) retrograde endoscopic lithotripsy and extraction, (3) percutaneousnephrolithotomy, (4) multimodal therapy, (5), percutaneousnephrostomy for chemical dissolution, and (6) open surgery (urethra, bladder, ureter, kidneys
Extracorporeal shockwave lithotripsy effective for stones smaller than 1.5 cm in diameter, stone-free rates are lower compared with rates for stones require 2-3 times the usual number of shocks to adequately fragment the stone. When considering candidates for ESWL, some authors suggest an upper limit of 1.5 cm for upper ureteral or renal cystine calculi. As reported by Kachel et al in 1991, these authors prefer to limit ESWL to renal calculi smaller than 1 cm in diameter.
Retrograde endoscopic lithotripsy and extraction . suitable for mid-to-distal ureteral cystine calculi when using high-energy modalities such as holmium:YAG laser or pneumatic shock devices (eg, Lithoclast). Smaller proximal ureteral calculi may also be treated in a retrograde fashion. Percutaneousnephrolithotomy the criterion standard for cystine renal calculi larger than 1-1.5 cm in diameter and for calculi for which ESWL or retrograde surgery has failed.
Multimodal therapy For large cystine stone burdens, such as occurs with full staghorn calculi, multimodal therapy may help achieve better stone-free rates. So-called sandwich therapy involves initial percutaneous ultrasonic lithotripsy followed by ESWL and then repeat ultrasonic lithotripsy or flexible nephroscopy and laser lithotripsy.
Percutaneousnephrostomy for chemical dissolution was successful in treating a limited number of patients in the late 1970s and early 1980s. The 2 most commonly used agents were -acetylcysteine (Mucomyst) A solution containing 60 mL of a 20% solution of N-acetylcysteine and 300 mEq of sodium bicarbonate per liter of saline is recommended. -tromethamine-E (THAM-E). an organic amine buffer with a pH level of 10.2. Treatment times range from weeks to months. relatively low success rates, rarely used today.
Open surgery Given the success of percutaneous nephrolithotomy, ESWL, and endoscopic retrograde approaches, open surgery is not indicated as first-line therapy for cystine calculi anywhere in the kidneys or ureter, with rare exceptions. Large bladder calculi may be amenable to open surgery, but these stones can also be treated with laser or electrohydraulic lithotripsy.
Conclusion Treatment of the patient with cystinuria requires close cooperation between the urologist and the nephrologist. Maintaining high diuresis of at least 3 L/d, regularly distributed throughout the night and day, even when sulfhydryl compounds are given, appears to be the major factor predictive of therapeutic success. Regular clinical, radiological, and biochemical surveillance appears to be of primary importance to maintain good long-term compliance with medical treatment.