Download
1 / 24
240 likes | 410 Views
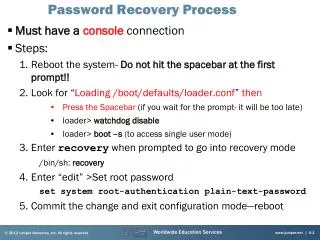
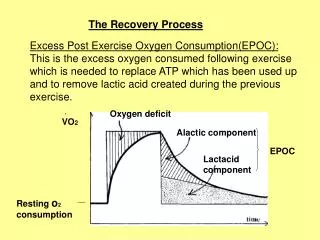
Intervening in the Recovery Process. Michael L. Dennis, Ph.D. Christy K Scott, Ph.D. Chestnut Health Systems, Bloomington &Chicago, IL U.S.A. Presentation in the National Institute on Drug Abuse’s (NIDA), Meeting on Treatment and Recovery Process , Bethesda, MD, January 15-16, 2004.

E N D
Intervening in the Recovery Process Michael L. Dennis, Ph.D. Christy K Scott, Ph.D. Chestnut Health Systems, Bloomington &Chicago, IL U.S.A. Presentation in the National Institute on Drug Abuse’s (NIDA), Meeting on Treatment and Recovery Process, Bethesda, MD, January 15-16, 2004. This presentation was supported by funds and data from NIDA and CSAT. The opinions are those of the author do not reflect official positions of the government
Dominant Paradigm of “Acute Care” Treatment and Research • Brief and/or short term single episodes of care focused primarily on substance use, motivation, cognition and coping skills • Indirect focus on changing the social recovery environment (with TCs being a major exception) • Minimal or no post-discharge check-ups • Evaluation of outcomes over relatively short periods of time (6-12 months) with the expectation that improvements should continue after treatment (i.e., an “acute care” model)
Current Conflicts with the Acute Care Model • Many consumers and clinicians view substance use as a chronic relapsing condition. • An emerging body of evidence from treatment epidemiology (e.g., DARP, TOPS, DATOS, UCLA, PENN, PETSA) suggests that the typical pathway to recovery currently involves multiple episodes of care over many years. • Among people admitted to publicly funded treatment reported in TEDS, for instance, 60% of the people had been been in treatment before (including 23% 1x, 13% 2xs, 7% 3xs, 17% 4 or more). • Attention has shifted from matching at intake to ongoing matching along a continuum of care based on the response to treatment. • Evaluation of outcomes is increasingly focusing on longer periods of time (2 to 5 years or more) and across multiple episodes of care.
This presentation will provide converging evidence from 2 studies that will demonstrate: • Substance use disorders are often chronic relapsing conditions, and • The feasibility of altering substance use trajectories and treatment careers using recovery management check ups and early re-intervention.
Study 1. Chicago Target Cities (CTC), Persistent Effects of Treatment Study (PETS), and Pathways to Recovery (Scott & Dennis) Recruitment: 1995 to 1997 Sample: 1,326 participants from sequential admissions to a stratified sample of 22 treatment units in 12 facilities, administered by 10 agencies on Chicago's west side. Levels of Care: Adult OP, IOP, MTP, HH, STR, LTR Instrument: Augmented version of the Addiction Severity Index (A-ASI) Follow-up: Of those alive and due, follow-up interviews were completed with 94 to 98% in annual interviews out to 7 years (going to 10 years); over 80% completed within +/- 1 week of target date. Funding: CSAT grant # T100664, contract # 270-97-7011 NIDA grant 1R01 DA15523
Intake Characteristics • Participants were mostly African-American (88%), female (59%), and in their 30s (48%); At intake, 32% were homeless and 25% were involved in the criminal justice system. • The most common substances used weekly were: cocaine (33%), heroin (31%), alcohol (27%), and marijuana (7%). • Many met criteria for Major Depression (36%) or Generalized Anxiety Disorder (36%). • 54% have been in treatment before (27% 2+ times) • The participants were initially referred to outpatient (19%), methadone (19%), intensive outpatient (18%), halfway house (10%), short term residential (20%), long term residential (13%).
Substance Use Careers Last for Decades 1.0 .9 .8 Cumulative Survival .7 Median duration of 27 years (IQR: 18 to 30+) Years from first use to 1+ years abstinence .6 .5 .4 .3 .2 .1 0.0 0 5 10 15 20 25 30
Substance Use Careers are Longer the Younger the Age of First Use Age of 1st Use Groups 1.0 .9 .8 Cumulative Survival .7 Years from first use to 1+ years abstinence .6 .5 under 15* .4 15-20* .3 .2 21+ .1 0.0 * p<.05 (different from 21+) 0 5 10 15 20 25 30
Substance Use Career are Shorter the Sooner People get to Treatment Year to 1st Tx Groups 1.0 .9 .8 Cumulative Survival .7 Years from first use to 1+ years abstinence 20+ .6 .5 .4 .3 10-19* .2 .1 0.0 0-9* * p<.05 (different from 20+) 0 5 10 15 20 25 30
Treatment Careers Last for Years 1.0 .9 .8 Cumulative Survival .7 Median duration of 8 years (IQR: 3 to 20) and 3 to 4 episodes of care Years from first Tx to 1+ years abstinence .6 .5 .4 .3 .2 .1 0.0 0 5 10 15 20 25
Over 55% Continued to Changed Status Between Annual Follow-up Interviews Status at 36 months Status at 24 months 100% 90% 80% In the community 70% In Recovery 60% 50% 40% In Treatment Incarcerated 30% 20% In the community 10% using 0% Recovery Inc. In Tx. In the Community Using (26%) (6%) (12%) (57%)
Study 2. Early Re-Intervention Experiment 1 (ERI-1) (Dennis & Scott) Recruitment: 2/00 to 4/00 Sample: 448 (84%) eligible adults sequentially admitted to Haymarket’s central intake Levels of Care: Adult OP, IOP, HH, STR, LTR, including PPW, Homeless, and Dual Diagnosis programs Instrument: Global Appraisal of Individual Needs (GAIN) Follow-up: Quarterly follow-up assessments were completed with 95-97% quarter between 3 and 24 post-intake; 100% of the participants completed 1 or more (82% completed all 8 follow-up assessments); over 80% completed with +/- 1 week of target date. Funding: NIDA grant # DA11323
Intake Characteristics • Participants were mostly African-American (84%), female (59%), and in their 30s (47%); at intake 27% were currently involved in the criminal justice system, 26% were homeless, and 25% of the females were or had been pregnant in the past year. • Dependence was most commonly on cocaine (71%), alcohol (39%), heroin (31%), and marijuana (9%). • Many had co-occurring internal disorders (75%) and/or external/impulse disorders (45%) • Most (68%) had been in treatment before (43% 2+ times) • The participants were initially referred to outpatient (7%), intensive outpatient (26%), short-term residential (45%), long-term residential (19%), or detoxification/other (2%).
Methods • Participants were randomly assigned to either an assessment Control group or the Recovery Management Checkup (RMC) group. • Research staff conducted face to face quarterly assessments with participants in both conditions over a 2-year time period. • All assessments were conducted using the Global Appraisal of Individual Needs-Intake (GAIN-I; Dennis, 1999).
Recovery Management Checkup (RMC) • Screening to determining “Eligibility” and “Need” • Linkage meeting/motivational interviewing to: • provide personalized feedback to participants about their substance use and related problems, • help the participant recognize the problem and consider returning to treatment, • address existing barriers to treatment, and • schedule an assessment. • Linkage assistance • reminder calls and rescheduling • transportation and being escorted
Median of 376 vs. 600 days, Wald=5.2, p<.05 Median of 376 vs. 600 days, Wald=5.2, p<.05 RMC (64% readmitted) H1: RMC Clients will return to treatment sooner 1.0 .9 .8 Percent to be Readmitted .7 .6 .5 Control (51% readmitted) .4 .3 OR: 1.34 X2(1)=6.8, p<.01 .2 .1 0.0 0 90 180 270 360 450 540 630 720 Days to Readmission
62 25% 50 17% H2: RMC clients will receive more treatment Days % with 90+ Days 70 30% 60 25% 50 20% 40 (months 4-24) Treatment (months 4-24) % with 90+ days of Subsequent 15% Mean Days of Subsequent Treatment 30 10% 20 5% 10 0 0% Control RMC Control RMC t(390)=2.65, p<.05 OR 1.61, X2(1)=4.1, p<.05
56% 43% H3: RMC clients will be less likely to use at 24m 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Control (n=244) RMC (n=224) X2(1) = 7.7, p<.01
Status Between Quarterly Follow-ups Has a Relatively Stable Distribution Over Time 100% 90% In the 80% community In Recovery 70% 60% In Treatment 50% Incarcerated 40% 30% In the 20% community using 10% 0% 0 3 6 9 12 15 18 21 24 Avg 3- 24 Months from Intake (n=448)
However, 32% of individuals change status between the beginning and end of the quarter In the community In Recovery In Treatment In the community using End of Quarter 100% 90% 80% 70% 60% 50% 40% 30% 20% Incarcerated 10% 0% Recovery Inc. In Tx. In the Community Using (42%) (5%) (12%) (41%) (3,136 quarterly transition Observations on 448 unique people) Beginning of Quarter
Multiple Pathways, with the Probability of Transition Varying by Initial State and Direction Probability of Entering Recovery is Higher from Treatment • Transition to Recov. • Freq. of Use (0.7) • Dep/Abs Prob (0.7) • Recovery Env. (0.8) • Access Barriers (0.8) • + Prob. Orient. (1.3) • + Self Efficacy (1.2) • + Self Help Hist (1.2) • + Days of Tx (1.2) 17% 18% In the Communit y In Recovery Using (76% stable) (71% stable) 27% 8% 33% 5% • Transition to Tx • Freq. of Use (0.7) • + Prob. Orient. (1.4) • + Desire for Help (1.6) • + RMC (3.22) In Treatment (35% stable)
Other Variables That Lost Significance in Multivariate Model • Problem Recognition, External Pressure, Internal Motivation, Treatment Resistance • Current Withdrawal, Number of Diagnosis, Emotional Problems, Illegal Activity, Homelessness • Coming from a controlled environment • Involvement with the Criminal Justice System, Mental Health, Health, or Training/School Systems • Lifetime number of prior treatment, arrests • Gender, Race, Age, Employment
Reprise • These studies provide converging evidence demonstrating that substance use disorders are of chronic relapsing conditions • That it is common for people to require multiple episodes of care, but that treatment is clearly an important factor in recovery. • That proactive monitoring and intervention can reduce the time to readmission, increase the amount of treatment and improve the long term probability of being in recovery
Contact Information • Michael Dennis Chestnut Health Systems, 720 W. Chestnut, Bloomington, IL 61701, 309-827-6026, e-mail: mdennis@chestnut.org • Christy K Scott Chestnut Health Systems, 712 N. Wells, 3rd floor, Chicago, IL 60610, 312-664-4321, cscott@chestnut.org