Download

1 / 40
750 likes | 2.72k Views
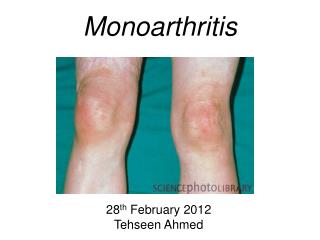
APPROACH TO MONOARTHRITIS. DR CB NEL. “ Inflammation of a single joint” Acute Chronic. WHERE IS THE INFLAMMATION?. ARTICULAR PERI-ARTICULAR pain all planes pain in plane of tendon active = passive active > passive

E N D
APPROACH TO MONOARTHRITIS DR CB NEL
“Inflammation of a single joint” • Acute • Chronic
WHERE IS THE INFLAMMATION? • ARTICULARPERI-ARTICULAR • pain all planes pain in plane of tendon • active = passive active > passive • capsular swelling/effusion linear swelling • joint line tenderness localised tenderness • diffuse erythema/heat localised erythema/heat
ACUTE MONOARTHRITIS • Septic arthritis • Crystal synovitis • Trauma • Haemarthrosis • Foreign body reaction • Monoarticular presentation of oligo- / polyarthritis • RA • Erythema nodosum • Juvenile idiopathic arthritis • Reactive, Psoriatic or other Seronegativespondiloarthropathy
CHRONIC MONOARTHRITS • Foreign body • Infection-Tuberculosis • Ch. Sarcoidosis • Enteropathic Arthritis (mainly Crohn’s) • Amyloidosis • Pigmented villonodularsynovitis • Synovial pathology (sarcoma, chondromatosis) • Monoarticular presentation of oligo- / poly articular disease
Crystal-induced Arthritis • Gout (monosodium urate crystals) most common - First MTP, ankle, midfoot, knee (can be any joint though) - Most initial attacks affect a single joint - Fever (more common with polyarticular) can raise suspicion for infection - Presence of crystal does not exclude infection - May see desquamation of overlying skin - Thiazide diuretics can put at risk - Needle shaped, negatively birefringent crystals • Calcium pyrophosphate dihydrate/pseudogout - Clinically not able to distinguish from gout - Most common in knee and wrists - Evolves over several days (less acute than gout) - Rhomboid shaped, positively birefringent crystals • Other crystals: apatite, calcium oxalate, liquid lipid
URIC ACID POOL Endogenous Exogenous Excretion Kidneys (2/3) Intestines(1/3) Serum urate: 0,12 - 0,55mmol/l Urine urate excretion: 1,5 - 4,4mmol/24 hours
MECHANISM OF HYPERURICAEMIA • Underexcretion(Most common) • Overproduction
HYPERURICAEMIA AND GOUT • Disorder of purine metabolism • Characterised • hyperuricaemia • deposition of uric acid or urate crystals in the tissues • Manifestations • acute attacks of gouty arthritis • tophi • kidney stones • urate-nephropathy
PATHOGENESIS • Hyperuricaemia causes gout, but is not synonomous with gout • Factors promoting crystallisation (0.55mmol/l) • the level of saturation • solubility • pH and temperature of the limb(colder areas)
PATHOGENESIS Crystallisationinjoint CrystalabsorbedbyPMN Secretion lysozyme enzymes Severe synovitis
ACUTE GOUTY ARTHRITIS • INCIDENCE • Mostly men > 40yrs • Association with Metabolic syndrome • Sometimes postmenopausal women • (Often on Diuretics)
PRECIPITATING CAUSES IN ACUTE GOUTY ARTHRITIS • Trauma and surgery • Medication • Alcohol • Diet
CLINIAL PICTURE ACUTE GOUTY ARTHRITIS • Goes to bed healthy • Wakes up sudden monoarthritis ( 85% Podagra) • (heel, instep, knee, wrist and hands and elbow -olecranon bursitis) • Rigors with severe pain • Night spent in torture • Joint is red (“ripe tomato”),warm and very tender. • After attack skin around the joint often peels off • Acute attacks usually pass completely until the next attack Uncontrolled hyperuricaemia may lead to polyarticular gout
DIAGNOSIS OF GOUT • Family history, as well as a typical history of attacks • Typical clinical picture and tophi • Elevated serum urate - (may be normal during attacks) • Urate crystals in aspiration fluid (as well as tophi) • X rays: Punched-out erosions (Rat bitten)
TREATMENT • Exclude precipitating causes • Increased water intake 2-3l/day • A low purine diet and avoidance of alcohol are recommended • Foods with a very high purine content: anchovy, sardines, liver and kidneys. Most meats, fish and chicken products also have a high purine content. • Treatment of associated conditions such as • obesity • Hypertension • Diabetes mellitus • hyperlipaemia • kidney failure
RX ACUTE ATTACK • Avoid prescribing prophylactics (uric acid lowering drugs) • NSAIDS ( not used in kidney failure) • Colchicine • Corticosteroids (in resistant cases)
Progression in the disease • Asymptomatic hyperuricaemia • continues until possible first attack • Acute gouty arthritis • Interval hyperuricaemia • periods between attcks • Chronic tophaceous gout • Complications • kidney stones and nephropathy
CHRONIC TOPHACEOUS GOUT • Deposition of uric acid crystals in the tissues (tophi) • After repeated attacks after 11 - 12 years • The tophi occur in • The auricles - helix • Tendons (hands, achilles tendon and feet) • Bursae - especially olecranon bursa • The tophi may ulcerate with secretion of pasty material
INDICATIONS FOR LONG-TERM PROPHYLACTIC THERAPY • If conservative measures do not have the desired effect and the levels still remain high (> 0.55 - 0.6 mmol/l) with repeated attacks • (If less than 1 attack per year is experienced, treatment is not necessary) • Positive family history of gout and kidney stones with very high urate levels • Chronic tophaceous gout • Kidney stones or nephropathy
MEDICINES FOR LONG-TERM PROPHYLAXIS • Allopurinol 300mg-900mg/day • Uricosurics medicines • Probenecid 250mg bd • Mustnot be used if there is kidney failure or kidney stones • To avoid kidney stones a high fluid intake (2l/day) must be maintained and in addition the urine can be alkalised with something like “citrosoda” • Colchicine 0.5mg should be added once or twice daily for the first few months in order to prevent recurrent attacks
CAUSES • Bacterial Gonococcal Non-gonococcal(Staphylococcus aureus , nongroup-A beta-hemolytic streptococci, gram-negative bacteria, and Streptococcus pneumoniae) • Viral – HBV, Rubella, Mumps, I.M, Parvovirus, Enterovirus, Adenovirus • Fungal
CAUSES • Most serious cause of monoarthritis, can destroy cartilage in one to two days • Non-gonococcal are most serious - most common in knees and hips - sternoclavicular joints in IV drug users - most febrile but do not appear especially ill - 90% monoarticular, hematogenous spread - 80% Gram(+) anaerobes * 60% S. Aureus (most PCN, some meth resistant) * 15% Non-group A, beta-hemolytic strep * 3% Strep pneumo - 18% Gram(-) - Anearobes on rise in IV drug users/immunocompromised/HIV
common organisms Staphylococci or Streptococcus young adults, significant incidence gonococcal arthritis Elderly & immunocompromised gram -ve organisms Anaerobes more common with penetrating trauma
Risk factors • Pre-existing joint disease • Prosthetic joints • Low SE status, IV drug abuse, alcoholism • Diabetes, steroids, immunosuppression/HIV • Previous intra-articular steroid injection
DIAGNOSIS • Synovial fluid aspiration • Volume/viscosity/cellularity/appearance • Gram stain/culture • Absence of organism does not exclude septic arthritis • Polarised light microscopy (crystals). Crystals don’t exclude septic arthritis. • NB suspected prosthetic joint sepsis should ALWAYS be referred to orthopaedics
DIAGNOSIS • Always blood cultures • Significant proportion blood cultures + ve in absence of + ve synovial fluid cultures • FBC ESR & CRP • BUT absence of raised WBC, ESR or CRP not exclude diagnosis of sepsis - if clinical suspicion high always treat
Antibiotic treatment of septic arthritis • Local and national guidelines • Liaise with micro. guided by gram stain • Don’t wait for cultures to start empiric antibiotic treatment • Conventionally given iv for 2 weeks or until signs improve, then orally for around 4 weeks
Joint drainage & surgical options • Medical aspiration, surgical aspiration via arthroscopy or open arthrotomy • Suspected hip sepsis – early orthopaedic referral – may need urgent open debridement