Download
1 / 56
650 likes | 882 Views
Key Components of a Successful Telephone Triage System. The Experience at an Integrated Wellness Center Rachel Ossmo, RN, BSN, David deBoer, PhD, Mona Dugo, LCSW and Teresa Carey, RN, BSN. Lakeshore Campus. ( 7.4 mi). Water Tower Campus. (12.8 mi). Health Sciences Campus.

E N D
Key Components of a Successful Telephone Triage System The Experience at an Integrated Wellness Center Rachel Ossmo, RN, BSN, David deBoer, PhD, Mona Dugo, LCSW and Teresa Carey, RN, BSN
Lakeshore Campus (7.4 mi) Water Tower Campus (12.8 mi) Health Sciences Campus
Nation’s Largest Jesuit Catholic University Total Student Enrollment ~ 16,000 Undergraduate ~9,800 - Graduate ~6,100 Full time student s ~ 13,500 Part time students ~ 2,500 On-campus students ~ 10,300 Commuter Students ~ 3,200 All Freshman and Sophomore students are required to live on campus unless given a special exemption to do otherwise Loyola University Chicago
LUC – Wellness Center • Integrated Model • Medical, Mental Health and Health Promotion • Staff of 30 people • Total of 23 FTE • Myriad of student workers, student trainees &Wellness Advocates Hours of Operation Academic YearSummer/Winter Break/Spring Break 8a – 6p Mon –Th. 8:00a – 4p Mon-Fri. 8a – 5p Fri. Closed Sat and Sun. 8a – 12p Sat.
Insurance • Coordinated and chosen through the Bursars office • Required by LUC for all full time students • Students can waive out of University plan and get coverage elsewhere if they choose. • WC does not bill for or make claims to insurance companies
Telephone Triage, Defined: “An interactive process between nurse and client that occurs over the telephone and involves identifying the nature and urgency of client health care needs and determining the appropriate disposition.” Telehealth Nursing Practice Core Course Syllabus AAACN.Org
Why Telephone Triage? “There is considerable evidence that telehealth interventions can decrease the cost of patient care while maintaining or improving both the quality of care and patient satisfaction. As issues of cost, shortages of nurses, and inadequate patient access continue to press, telehealth must be among the approaches the nurse leader considers as she works to construct viable current and future health care options.” Jean Sorrells-Jones, Poldi Tschirch, Marie Anne S. Liong, Nursing and telehealth: Opportunities for nurse leaders to shape the future, Nurse Leader, Volume 4, Issue 5, October 2006, Pages 42-46,58, ISSN 1541-4612, 10.1016/j.mnl.2006.07.008.
Desired Outcomes Immediate access to an RN Increase utilization of Telephone Triage line Refer to most appropriate provider Decrease call volume at front desk
Steps for Implementation Developed telephone triage protocols Installed a voice mail prompt Staffed line with RN during all clinic hours Medical staff completed triage re-training session Posted advertising on Wellness Center website Evaluated and updated telephone triage documentation forms (before EMR)
Adapting to Student’s NeedsEvolution of Making an Appointment
NCHA Data 2010 Proportion of college students who self reported being diagnosed or treated by a professional for the following:
Nearly 50% of College Health Concerns Addressed in Telephone Triage
Benefits Contributing to Student Learning Outcomes 1. Students will demonstrate health literacy2. Students will identify risk reducing behaviors that promote a healthy community3. Students will demonstrate self-care skills that promote academic success.
Learning Outcome #1 • Students will demonstrate health literacy. • Resource for follow-up questions • Referrals and insurance issues
Learning Outcome #2 • Students will Identify risk reducing behaviors that promote a healthy community. • Antibiotic education • Sexual Health Issues • Preventative Care
Learning Outcome #3 • Students will demonstrate self-care skills that promote optimal health to enable academic success. • Access to knowledge • Time friendly
Additional Benefits • Identifying an emergent call • Pt is triaged prior to appt • Better Use of Services and Time • Reduced Walk-in appointments • Increases availability of same day appointments • More efficient and effective use of office time
Benefits • Encourages Autonomy • Patient Education • Self-care guidance • Continuity of Care • Better time management • Increase Patient Compliance
Benefits • Increased Patient Satisfaction “The creation of a ‘telephone clinic’ which utilizes nurses and house staff physicians trained and dedicated to telephone communication directly with patients resulted in more efficient management and greater satisfaction for patients.” - Patient Educ Couns. 2010 Sep;80 (3): 351-3 Epub 2010 Aug 4 “If your visit today was preceded by a brief telephone call with a Wellness Center nurse or counselor, did this call help you know what to do next?” LUC Wellness Center Student Satisfaction Survey
Challenges • Staffing • Access • Potential for Error • Missed Opportunities
Using our EMR to provide written materials Teaching sheets Referrals Secure messages Adapting
RN has access to MH notes Can direct calls to appropriate provider in a timely manner Can also alert MH provider if there is a specific concern about a pt. Collaborating with MH
After hours RN Advice Line Phone # left on VM at close Next day report Other LUC departments Dean of Students Campus Safety Collaborating Outside the Wellness Center
Multi-tasking – what nurses do best Collaborating Outside the University
Track how many appointments are made as a result of triage calls Track the work that is being done in DAN but not being accounted for now. Surveying all triage calls for satisfaction rather than just those patients who were actually seen For the Futureof Triage
Screening Healthy Lifestyle Questionnaire Brief Past Medical History Survey Gives opportunity to check in with pt in other areas: Nutritional, mental, sexual and social health. Can answer questions, make referrals and set up appts in these other areas during the appt
PHQ - 2 Patient Health Questionnaire Depression Module Developed by Kroenke, Spitzer and Williams Brief measure of depression often used as part of a past medical history questionnaire Two-item survey whose questions are derived from symptoms for a DSM-IV diagnosis of major depression Medical Care. Vol. 41, Number 11, pp 1284-1292. 2003. Lippinott,Williams and Wilkins, Inc.
PHQ-2 • Research has demonstrated that over 82% of patients with major depression score a three or greater • Initial counseling visit is always offered at WC when patient scores a 3 or greater
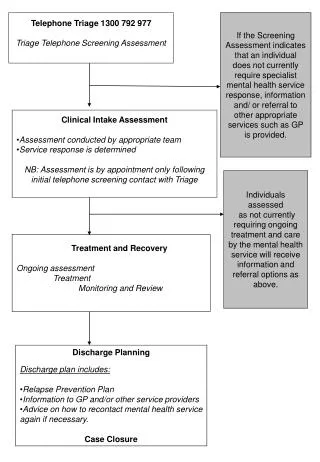
Evolution toward Mental Health Telephone Triage • Traditional Intake Model • Day-time coverage hours
Benefits of Old System • 60 minutes, thorough assessment • In person; facilitated rapport, easier to assess nuances • Clinical intervention along with assessment
Challenges of Intake Model • Up to 10-day lag time between initial call and first contact • Flip side of rapport--face-to-face contact at times made it more difficult to refer out; referral to another internal therapist could be frustrating for clients • Paperwork burden • Higher no-show rate
What we hoped to achieve • Improved efficiency, reduce waitlist • Reduce paperwork burden e.g. intakes referred out • Advance the time of first patient contact • Improve responsiveness to campus partners • Increase/expedite referrals to the community • Shift burden from nurse triage line and MH coverage phone • Avoid intakes on ADHD issues
Rollout Process • Administrative planning • Helpful guiding resource: Rockland-Miller, H.S. & Eells, G.T. (2006). The implementation of mental health clinical triage systems in university health services. Journal of College Student Psychotherapy, 20(4), 39-51. • Consultation • Staff Discussion, input, planning • Implemented Fall 2010 on pilot basis
Web based booking Dial a nurse Front desk staff Mental health coverage worker Booking a triage appointment
Referred for therapy at Wellness Center Refer out for therapy Waitlist Routine appointment Priority appointment Urgent appointment Emergency appointment Psychiatry appointment Group referral Disposition from Triage
Database of community providers Long term/chronic conditions Not in acute distress Previous experience with therapy Demonstrates good insight and high degree of motivation for long term therapy Has insurance or financial means for care Wait list Referring out:
First experience of therapy Acute state of distress Cultural barriers to therapy Lack of family support Short term treatment appropriate Referred by campus partner Financial barriers Eating Disorder Likely to be scheduled at WC