Download
1 / 121
1.22k likes | 1.44k Views
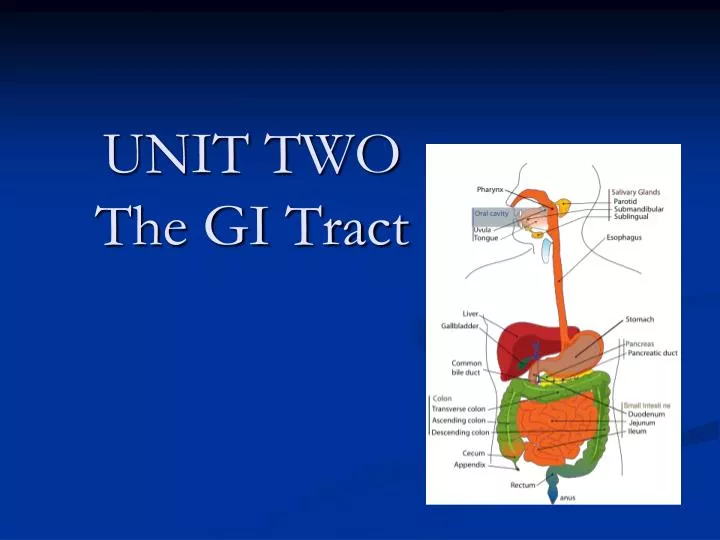
UNIT TWO The GI Tract. Gastro-Intestinal Tract & Disorders. Objectives. Review the A&P of the GI system Discuss the significance of vitamins and our ability to absorb them Describe oral infections/inflammations and the nursing care.

E N D
Objectives • Review the A&P of the GI system • Discuss the significance of vitamins and our ability to absorb them • Describe oral infections/inflammations and the nursing care. • Discuss the pathophysiology of esophageal disorders and the treatment /nursing care (i.e. GERD, hiatal hernia) • Discuss the pathophysiology of disorders of the stomach and upper small intestine (i.e. gastritis, upper GI bleed, peptic ulcer disease).
Selected Readings • In Your text chapters chapters 34, 35, 36, 37 • Readings from your syllabus
Can you imagine: • Not to be able to eat anything with wheat in it? What condition? • What it is like to live with an esophageal sphincter not closing? What condition? • Living with part of your stomach in your esophagus? • Being incontinent of stool or continuous diarrhea? • Open Sores over your lips on most important occasions...
The main functions of GI system: • Ingestion & propulsion:(movement )food done by mouth, pharynx , esophagus • Digestion(mouth, stomach, small intestine) • Absorption(mouth, stomach, small intestine) • Elimination(large intestine) • GI organs: liver, biliary tract & pancreas.
Mouth & Ulcerative Colitis /Crohn’s &Celiac
Food & GI System: Food generally takes about four hours to make it from the mouth to the end of the small intestine. The non-digested residue normally spends one to three days in the large intestine but can be there for seven days. Foods high in insoluble fiber (whole grains, wheat and corn brans, some vegetables) speedup intestinal transit. This is desirable because it prevents constipation, hemorrhoids, and diverticular disease.
Vitamins Fat Soluble (stored & need fat for absorption): • A: vision (fish, fruit, veg) • D: bone (dairy products esp calcium) • E: Antitoxins (dairy) • K: Blood clotting (milk, gr leafy veg) Water Soluble (not stored): • C: Connective tissue ascorbic acid, citrus, gr veg, tomatoes, broccoli • B1, B2,B6, B12: energy, lips, GI, RBC, heart, skin, gait, eyes synthesis DNA/RNA (meat veg, dairy products) NB: Vitamin B12 needs intrinsic factor
Vitamin B12 • Acts as antitoxidant • Essential to formation of the protein collagen • facilitates iron absorption • facilitates cholesterol conversion to bile acids • essential to serotonin synthesis
Intrinsic factor • Parietal cells in the stomach secrete the the intrinsic factor necessary for the absorption of vitamin B12 in the small intestine. • A lack in Vitamin B12 results in pernicious anemia. • Loss of intrinsic factor also leads to degeneration of nerves & spinal column
Oral Inflammations & Infections: • The person who is ill, on medication, or receiving radiation is subject to alterations in ecology of the mouth & subsequently to decay, periodontal disease, and injury to the oral mucosa. • Identify oral stressors: mechanical, chemical, infectious, or due to local or systemic disorder
St. Vincent’s Oral Candidiasis Herpes Simplex I Cold Sore Stomatitis Gingivitis Parotitis
Oral Candidiasis Care: • Candidiasis: topical nystatin suspension (2 ml four times a day) or miconazole gel (5-10 ml four times daily, held in the mouth with dentures removed). • Resistant candidacies: usually responds to systemic oral fluconazole (50 mg capsule daily for 7-14 days). • Very frequent mouth care is essential
Herpes SimplexThis close-up view of early herpes outbreak shows small, grouped blisters (vesicles) and lots of inflammation (erythema).
Transmission HSV: Herpes is most easily passed through inoculation from active lesions. The virus may also spread during times when there are no symptoms, and from sites that are seemingly inactive. There is a significant percentage of genital herpes infections resulting from oral to genital sexual contact. Most of these oral to genital transmissions will be of the type 1 variety, although type 2 incidence is not uncommon.
General Nursing Interventions for Oral Pain Relief: • Careful, regular, frequent mouth care • Oral agents such as Lidocaine 2% viscous, Benadryl elixir, Antacid, & Kaopectate, Acetaminophen • Topical agents such as coating agents • Swishing agents providing topical & anti-inflammatory action analgesia • Iced water or a dish of crushed ice (with spoon). • Mouth sprays - a small hand-held spray filled with iced fruit juice is simple and effective. It can be easily used by client or relative • Artificial saliva - frequent sips of `artificial saliva' may help some patients. An artificial saliva aerosol spray such as An artificial saliva spray such as Moistir is also available.
Oral Cancer • Occur lips or anywhere within the mouth. • Smoking, excessive alcohol, chronic irritation from a jagged tooth, poor dental care, constant exposure to sun are predisposing factors • Usually appears painless ulcer on lip • Ca tongue ulcer or area of thickness, sore • Biopsy to diagnose • Treatment surgery, radiation, chemotherapy or combination.
Esophageal Disorders • Mechanical : Tumor, Diverticulum, injury • CV: aneurysm, varices • Neurogenic: Neuro, CVA
Esophageal Disorders • GERD (Gastroesophageal Reflux Disease) • Hiatal Hernia • Esophageal Cancer • Esophageal Diverticula • Esophageal Strictures • Achalasia • Esophageal Varices
Common Signs & Symptoms of Esophageal Disorders • Problem swallowing * • Pain * • Hoarseness * • Weight loss * • Bleeding * • Regurgitation (water brash) • Heart burn • Hiccups
GERD • Syndrome • No one single cause Factors causing GERD: • Impaired esophageal mobility • Delayed gastric emptying • Defective mucosal defense • Reflux of gastric contents • Lower Esophageal Sphincter (LES) dysfunction –main factor.
GERD Normally, after a meal, the lower esophageal sphincter (LES) usually remains closed. Secondary peristalsis returns approx. 90% of the acid and food to the stomach. Once peristalsis ends, the LES closes again. The remaining acid in the esophagus is neutralized by successive swallows of saliva, which is alkaline in nature - it is then cleared into the stomach. When LES relaxes at inappropriate time, it allows acid and food particles to reflux into the esophagus. (GERD)
Factors that Increase LES Pressure: • Reglan • Urocholine • Motilium • Gastrin • Nonfat milk • Chewing gum helps GERD
Some Common Agents that Decrease LES Pressure: • Alcohol, Nicotine, ASA • Anticholenergic drugs • Beta-adrenergetic blocking drugs • Calcium channel blockers • Chocolate, Coffee, Fatty foods, Peppermint • Demerol, Estrogen, Lidocaine, Morphine hinders GERD
Clinical Manifestations GERD • Heartburn very common due to gastroesophageal reflux • chest pain • Respiratory systems- wheezing, coughing, dyspnea • Otolaryngologic symptoms- hoarseness, sore throat, feeling as though a lump in throat, choking • Regurgitation common • Gastric symptoms- early satiety, post meal bloating, N&V.
Complications of GERD • Esophagitis • Barrett’s esophagus • Respiratory complications: bronchospasms, laryngospasms, pneumonia • Dental erosion
Diagnosing GERD • Barium swallow /X-ray if protrusion upper part of stomach • Esophageal Endoscopy • Biopsies to determine ca stomach or Barrett’s esophagus • Esophageal manometric studies- measure pressure esophagus & LES • PH measuring devices to determine if acid in esophagus • High-dose proton pump inhibitor (PPI)
Esophageal Endoscopy • NPO 6-10 hours pre examination. Why? • Why is a local spray anesthetic used? • Why suction & CPR equipment ready? • Why withhold fluid & food post exam? • How long? • What can you do for throat discomfort? • What do you check for post procedure?
Nursing Interventions for GERD • Assess cause • Position-elevate head no lying down 2-3 hrs. post eating • Nutrition • Drugs as ordered • Lifestyle- stop smoking, Weight loss
Drugs for GERD: Drugs for GERD focus on: • Improving LES function (urecholine) • Increasing esophageal clearance (metoclopramide) • Decreasing volume & acidity of reflux (H2 receptor blockers, PPI, maalox, mylanta) • Protecting esophageal mucosa (gaviscon, carafate) • If they do not work surgery maybe required
Angelchick antireflux Surgery B Menu F