Download
1 / 91
910 likes | 1.06k Views
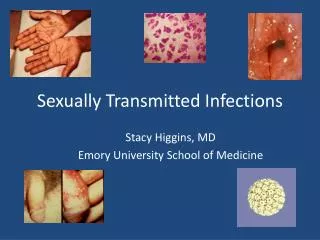
Sexually Transmitted Diseases, Part II: Genital Syndromes in Women Dr. Devika Singh, MD, MPH June 4, 2009 Slides generously borrowed from mentor Jeanne M. Marrazzo, MD, MPH. STD as a Cause of Cervicitis and Ulcerative Disease. Endocervicitis: ‘classic’ STD pathogens Gonorrhea

E N D
Sexually Transmitted Diseases, Part II: Genital Syndromes in Women Dr. Devika Singh, MD, MPH June 4, 2009 Slides generously borrowed from mentor Jeanne M. Marrazzo, MD, MPH
STD as a Cause of Cervicitis and Ulcerative Disease • Endocervicitis: ‘classic’ STD pathogens • Gonorrhea • Chlamydia trachomatis • Ectocervicitis: often associated w/ vaginitis: • Trichomoniasis • Discrete lesions/Genital ulcerative disease/myriad • Herpes simplex virus • Syphilis • Chancroid • Human papillomavirus • LGV
Things to Consider • Age of patient • Change in discharge: increased, malodorous, bloody, purulent • Associations: sexual activity/partnerships, cleaning the vagina (including douching/irrigation) • Co-infections: HIV or non-HIV • Epidemiology/exposures
Case I 22 yo woman presents to your clinic. She endorses no particular symptoms. One male partner who is asymptomatic. Condoms used “sometimes” On no hormonal contraception
Differential? • Chlamydia trachomatis • Neisseria gonorrhoeae • HSV • HPV • Trichomoniasis • Syphilis • Pregnancy
Chlamydia trachomatisEpidemiology • Most common bacterial STD worldwide, with approximately 90 million cases each year • Uro-genital disease • Ophthalmologic • Invasive (Lymphogranuloma Venereum) http://www.who.int
Clinical Syndromes Caused by C. trachomatis Conjunctivitis Urethritis Cervicitis Proctitis Endometritis Salpingitis Perihepatitis Infertility Ectopic pregnancy Chronic pelvic pain Women Conjunctivitis Pneumonia Pharyngitis Rhinitis Infants Chronic lung disease (?)
C. trachomatis Cervical Infection • Classic cause of endocervicitis • Mucopurulent discharge • Friability • Edematous ectopy • Cervical signs occur in minority of patients (10-20%) • Most (80-90%) infected women have normal cervix / no signs
General Characteristics of Chlamydia • Superficial, mucosal: epithelial cells • Often no (or minimal) signs or symptoms • Chronic in women (months to years) • Chronic inflammatory response • Serious reproductive sequelae in women • Reinfection common www.pasante.com
Normal Fallopian tubes by Scanning EM Photos courtesy of Dorothy Patton, PhD
Fallopian tubes by EM after C. trachomatis infection Photos courtesy of Dorothy Patton, PhD
Chlamydia Tests • Cell culture • Antigen Detection • Direct Fluorescent Antibody (DFA) • Enzyme Immunoassay (EIA) • Unamplified DNA Probe (Gen Probe PACE2) • Signal Amplification Tests (Digene Hybrid Capture) • Nucleic Acid Amplification (NAAT) • Rapid Point of Care Tests
What is the recommended treatment for a pregnant woman with chlamydia? • Erythromycin 500 mg po QID x 7 days • Doxycycline 100 mg po BID x 7 days • Azithromycin 1 g po x 1 dose • Levofloxacin 500 mg po daily x 7 days
Chlamydia Treatment in Pregnancy 2006 • Recommended regimens • Azithromycin 1 g PO x 1 • Amoxicillin 500 mg PO TID x 7 d • Alternative regimens • Erythromycin base 500 mg PO QID x 7 d • Erythromycin base 250 mg PO QID x 14 d • Erythro ethylsuccinate 800 mg PO QID x 7 d • Erythro ethylsuccinate 400 mg PO QID x 14 d
2006 CDC STD Treatment Guidelines:Uncomplicated Chlamydial Infection • Recommended • Azithromycin 1 g PO, single dose, directly observed • Doxycycline 100 mg PO BID x 7 d • Alternatives • Ofloxacin 300 mg PO BID or • levofloxacin 500 mg PO qD x 7 d • Erythromycin 500 mg PO QID x 7 d
Counseling as Part of Chlamydia Treatment • Abstain for at least 7 days and until partner(s) treated • Consistent condom use • Get your partner treated • Return if not improved over next 7-14 days
A Word about Screening UNITED STATES • <24 years old: screen all sexually active women annually • 25 and older: Annual testing if ‘at increased risk’ • Defined liberally: inconsistent condom use, new or multiple partners, prior STD or CT, sex work, certain demographics • If pregnant: • <24 years old screen • 25 and older – only screen if “at increased risk”
Chlamydia Proctitis LGV strains Severe Proctocolitis Blood, ulcers, pus Granulomas Increased (>1/64) Non-LGV Mild Proctitis Normal, pus PMNs Normal • Severity • Extent • Sigmoidoscopy • Biopsy • Comp-fix AB
LGV (Serovars L1, L2, L3 of Chlamydia) Proctitis Biopsy showing crypt destruction by diffuse histiocytic and lymphocytic infiltrate • Settings: developing context traditionally, but trend recently has included West (MSM) • Diagnosis • Cell culture OK if available • NAAT not cleared by FDA for rectal specimens • Can be used if validated by local laboratory • ID of LGV serovars requires culture serotyping or NAAT genotyping; neither widely available • Serologic tests: recommended, but @reference laboratories; titers not well-defined for LGV proctocolitis and not highly predictive of infection Ratelle; Liu 2006 www.cdc.gov/std/lgv
LGV (Serovars L1, L2, L3 of Chlamydia) Proctitis • Consider presumptive treatment • Doxycycline 100 mg bid PO x 21 d Ratelle; Liu 2006 www.cdc.gov/std/lgv
Chronic lymphogranuloma venereum in female. Genital elephantiasis
Case II • 33 yo woman presents with change in vaginal discharge. • One new male sex partner for past three months. Previously was with one steady male partner x four years.
Regardless… • ALWAYS do an examination • Presumptive treatment is inappropriate
Purulent cervicitis When seen, tends to be MOST likely • C. trachomatis • N. gonorrhea
Gonorrhea Treatment, 2007 • Recommended regimens: • Ceftriaxone 125 mg IM x 1 • Cefixime 400 mg PO x 1 • Ciprofloxicin 500 mg PO x 1 • Ofloxacin 400 mg PO x 1 • Levofloxacin 250 mg PO x 1 Alternative regimens: • Cefpodoxime 400 mg po x 1 • Cefuroxime 1 g po x 1 • Spectinomycin 2 g IM x 1: not available • Single-dose injectable cephalosporin regimens • Single-dose oral quinolone regimens Co-treat for chlamydia unless ruled outwith highly sensitive test (NAAT) MMWR April 13, 2007; 56 (14)
Case III • 37 yo woman presents with pain while having intercourse with her husband. • She denies any vaginal discharge. • He is asymptomatic.
Bartholin’s abscess Aerobic organisms Neisseria gonorrhoeaeStaphylococcus aureusStreptococcus faecalisEscherichia coli Pseudomonas aeruginosChlamydia trachomatis Anaerobic organisms Bacteroides fragilisClostridium perfringensPeptostreptococcus speciesFusobacterium
Treatment • Placement of Word catheter • Culture/analysis fluid to ensure no co-infection or other findings (rarely, malignancy) • Treatment is generally broad-spectrum (including for C. trachomatis and N. gonorrhea)
Case IV 24 y.o. woman presents with increased, malodorous vaginal discharge for 5 days. She has two sex partners: one man and one woman She practices no safe sex precautions
Trichomoniasis • Single-celled protozoan parasite, Trichomonas vaginalis. • The vagina is the most common site of infection in women, and the urethra (urine canal) is the most common site of infection in men. http://www.cdc.gov/STD/Trichomonas
Trichomoniasis • The parasite is sexually transmitted through penis-to-vagina intercourse or vulva-to-vulva contact with an infected partner. • Women can acquire the disease from infected men or women, but men usually contract it only from infected women. http://www.cdc.gov/STD/Trichomonas
Trichomoniasis • Signs or symptoms of infection which include a frothy, yellow-green vaginal discharge with a strong odor. • May cause discomfort during intercourse and urination, as well as irritation and itching of the female genital area. In rare cases, lower abdominal pain can occur. Symptoms usually appear in women within 5 to 28 days of exposure.
Trichomoniasis Treatment 2006 • Recommended regimen: • Metronidazole 2 g PO x 1 • Tinidazole 2 g po x 1 • Alternative regimen: • Metronidazole 500 mg PO BID x 7d • Metronidazole safe at all stages of pregnancy; tinidazole Category C (don’t use) • Vaginal therapy is ineffective • Treat sex partner(s): male and female
Case V 28 y.o. woman comes to your clinic because she has noted increased, malodorous vaginal discharge for about a week. No history of known STD. In your history you note that she washes her vagina with a “special rinse” every month She has been monogamous with a male partner, who is asymptomatic, for 1 year.
Case V She and her sex partner do not use condoms on most occasions but practice “withdrawal” method.
What do you advise? • She probably has a yeast infection because she is at low STD risk • She probably has trichomoniasis, and you’ll call in a prescription for tinidazole/metronidazole. • Come in for examination. • Stop irrigating vagina