Download
1 / 57
870 likes | 1.83k Views
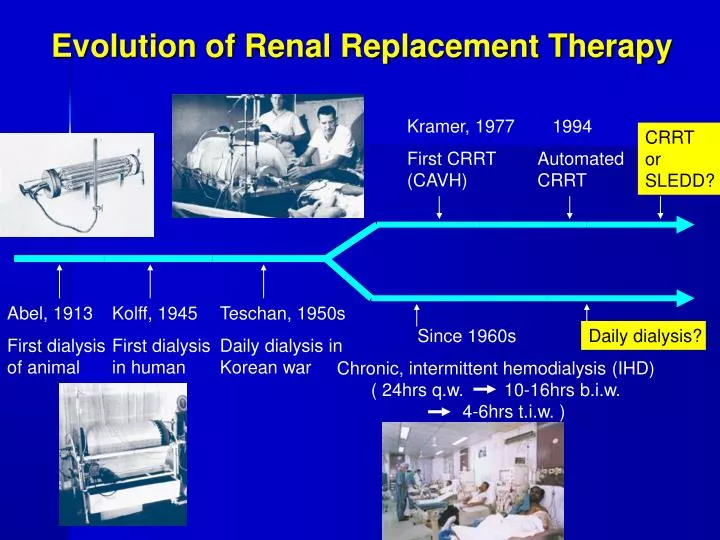
Evolution of Renal Replacement Therapy. Kramer, 1977 First CRRT (CAVH). 1994 Automated CRRT. CRRT or SLEDD?. Abel, 1913 First dialysis of animal. Kolff, 1945 First dialysis in human. Teschan, 1950s Daily dialysis in Korean war. Since 1960s

E N D
Evolution of Renal Replacement Therapy Kramer, 1977 First CRRT (CAVH) 1994 Automated CRRT CRRT or SLEDD? Abel, 1913 First dialysis of animal Kolff, 1945 First dialysis in human Teschan, 1950s Daily dialysis in Korean war Since 1960s Chronic, intermittent hemodialysis (IHD) ( 24hrs q.w. 10-16hrs b.i.w. - 4-6hrs t.i.w. ) Daily dialysis?
Basic Principle of Renal Replacement Therapy NEJM 336:1303-1309
IL-6, TNF-α IL-6 20000 Molecular weights cut-offs <30000> IL-1, IL-8 IL-1, IL-8, TNF-a
Clearance = QF x SCQF= filtration amount SC=sieving coefficients
Hemodialysis NEJM 336:1303-1309
Hemofiltration NEJM 336:1303-1309
Component of renal replacement therapy • Membrane • Vascular access • Anti-coagulant • Dialysate • Renal replacement fluid
Choice of membrane • Substituted cellulose dialyzers : • hydroxyl group • Cellulose acetate, diacetate, triacetate • Synthetic dialyzers : • Polysulfone (PS) • Polyamide (PA) • Polyacrylonitrile (PAN) • Polymethylmethacrylate (PMMA) American Journal of Kidney Disease, Vol 35, NO 5(May), 2000:pp980-991
Choice of membrane • Biocompatible membrane (activate less complement and greater higher 2-microglobulin clearance, greater hydraulic permeability.low and high-flux synthetic membranes) • Hypotension and prolongation of ARF in biocompatible membranes • Adsorptive vs. nonadsorptive membrane in CRRT American Journal of Kidney Disease, Vol 35, NO 5(May), 2000:pp980-991
Vascular access • Grade C : avoided subclavian in adults • Grade D : avoided femoral vein in neonates and young (femoral vein thrombosis is a significant problem) • Grade C : Internal jugular vein • Level II and III studies : Ultrasound guidance • Re-circulation is likely to be significant for blood flow in excess of 200 c.c/min, but depending on catheter design and location • The first international consensus conference on CRRT, 2002
Double lumen : Re-circulation rate under 250cc/min blood flow • Subclavian , internal jugular vein < 3% • Catheter length • Femoral vein 24cm : 10%, 15cm : 18% • Blood flow • 400 cc/min : 38% in the femoral vein American Journal of Kidney disease , 1996
Anticoagulation • Standard protocol • Initial bolus 10-30 unit/kg of heparin • Infusion 10-30 unit/kg to target • ACT :170-220 seconds or • PTT: 2 X N.J.Maxvold, T.E. Bunchman/Crit Care Clin 2003 19(2),563-575
Ideal replacement fluid/dialysate • Principle: remove waste, supply lost • Nearly plasma water • Supply inadequate component • Individualized • Different disease
Dialysate (透析液) Units: mEq/L
Hybrid therapies in ICU • CRRT (Continuous Renal Replacement Therapy ) • EDD ( Extended daily dialysis ) • SLEDD ( Slow Low-efficient Daily Dialysis ) • SLEDD-f (Sustained Low-efficiency Daily Diafiltration ) • IHD ( Intermittent Hemo-dialysis )
CRRT iHD
Hybridor Prolonged Intermittent Renal Replacement Therapies CRRT iHD
EDD: Extended Daily Dialysis • Fresenius 2008H delivery system • Double lumen • Toray 2.0 m2 dialyzer • Duration : 6 ~ 8 hrs • Blood flow : 200 ml/min • Dialysate flow rate : 300 (500) ml/min • Dialysate potassium concentration 4 meq/L • Dialysate bicarbonate concentration : 30 ~ 35meq/L American Journal of Kidney Disease, Vol 36, No 2 (August), 2000: pp 294-300
SLEDD( Slow Low-efficiency Daily Dialysis ) • Fresenius 2008H delivery system • Double lumen • Duration : 6 ~ 12 hrs • Blood flow : 200 ml/min • Dialysate flow rate : 300 ml/min • Dialysate bicarbonate concentration : 30 ~ 35meq/L American Journal of Kidney Disease, 2000
SLEDD-fSustained Low-efficiency Daily Diafiltration • Fresenius 4008S • Double lumen • Duration : 8 ~ 12 hrs • Blood flow : 200 ml/min • Dialysate flow rate : 200-300 ml/min • High Flux Dialyzer • Online replacement fluid Nephrol Dial Transplant 2004 19:877-887
HD treatment in ICU depend • Treatment behavior • Availability of treatment methods • Organization of the unit • Knowledge and experience of nurses • Existence of nephrological unit in the hospital • Cost • Individual doctor must therefore know the advantages and disadvantage of different treatment options Kidney Blood Press Res2003;26:123-127
Daily hemodialysis and the outcome of acute renal failure • ARF require CRRT is related high mortality and uremic damage to other organ systems • Intensive hemodialysis reduces mortality without increasing hemodynamically induced morbidity. • Survival was the primary endpoint of the study • Mortality rate : 28% Vs. 46% (daily H/D Vs. Alternate H/D ) N Engl J Med 2002;346:305-10
IHD vs CVVH Journal of the American Society of Nephrology, 2001
What is SLEDD-f ?? • Sustained Low-Efficient Daily Diafiltration • A conceptual and technical hybrid of continuous veno-veno hemofiltration(CVVH : convection) and intermittent hemodialysis (IHD : diffusion )
Advantage of SLEDD-f • Patient mobility ↑ • Anticoagulation ↓ • hemodynamic stability – or ↑ • Nursing labor ↓ • Professional ↑ • Cost ↓ American Journal of Kidney Disease, 2000
The predominant potential advantages of continuous renal replacement therapy • Hemodynamics stability correction of hypervolemia and metabolic acidosis • Better solute removal • Recovery of renal function • Biocompatibility • Correction of malnutrition • Better removal of cytokines • Overall outcomes ? Kidney Blood Press Res2003;26:123-127 Journal of the American Society of Nephrology, 2001
Potential disadvantages of CRRT • Need for continuous anticoagulation • More difficult drug dosing • Low efficiency interims of unit/ time ( e.g. Severe hyperkalemia) • Nonselective solute removal : depletion syndrome with prolonged use of high Qf ? The Netherlands Journal of Medicine August 2003
Sustained low-efficiency dialysis in the ICU: Cost, anticoagulation, and solute removal Treatment parameters for current and previous SLED studies KI (2006) 70, 963-968
Sustained low-efficiency dialysis in the ICU: Cost, anticoagulation, and solute removal Measures of small solute removal KI (2006) 70, 963-968
Sustained low-efficiency dialysis in the ICU: Cost, anticoagulation, and solute removal Daily and weekly cost of SLED and CRRT KI (2006) 70, 963-968
Dialysis guideline in NTUH SICU • Dominant and responsibility by Intensivist • Hybrid Therapies in NTUH SICU • Setting up and performing by Technician and NP
Guideline in CVVH Indication: (1). Cerebral edema:Mannitol ≧ q12hr in use frequency (2). Prevention of post-dialytic “ rebound” intoxication Setting: • Double lumen: 14Fr,儘量打在right neck vein • blood flow: 200mL/min • hemofiltration: 35mL/kg/hr • dialyzer: PAN 10 • HF-400 CVVH:pre-dilution : post-dilution= 50%:50% • Replacement fluid:信東A+(B+Rolikcan),若病人「K+」低,則每袋B液加KCl (20 meq)一支
Guideline in IHD (1). IHD (4 hr):病況穩定時使用之 (2). EDD (4 ~ 6hr):stable hemodynamics,但預計脫水超過2L,為了增加脫水量而延長H/D時Initial H/D setting for patients with double lumen • Blood Flow:200c.c/min • Dialyzer:FK-18C (EVAL 1.8m2) • Dialysate:IHD、EDD set 500c.c/min,SLEDD set 300c.c/min • Net UF rate: max 500c.c/hr, 若須更多的脫水,則延長透析時間 (EDD) • Dialysate Temp.:37℃ • Dialysate:信東No 9+GB solution
Guideline in SLEDD、 SLEDD-f Indication: 取代CVVH • blood flow: 200mL/min • Dialysate: 300mL/min,Dialysate Temp. : 38℃ • Portable RO機使用 • Dialyzer: FX60 (FMC, Helixone 1.4m2) • Duration:8 ~ 12hr • Replacement fluid:UF rate : 35c.c/kg/min • Dialysate:信東No 9+GB solution
Guideline in heparin use Priming solution:2000 unit/1000c.c N/S 以下情況不用Heparin: • Major operation 48 hr • Bleeding tendency:INR>2.0 or PTT > 50sec or Plat 50000 • Active bleeding:e.g. GI bleeding, Surgical bleeding, etc • 其他情形使用heparin • Heparin solution concentration: 2c.c heparin (10000 unit)/20c.c N/S • Dosage:30 unit/Kg/hr • H/D結束前1小時,停止Heparin infusion Reference: Journal of Nephrology 2003:6;566-571