Download
1 / 30
300 likes | 358 Views
A Study on the Relative Efficiency Of Colorectal Endoscopists. Barbara Lum Nathan Hedges Ruwan Kiringoda Sarah Hong. Colonoscopy. Colonoscopy is the best technique for examination of the large intestine, and for the biopsy and treatment of mucosal lesions. Data Source for the Project.

E N D
A Study on the Relative Efficiency Of Colorectal Endoscopists Barbara Lum Nathan Hedges Ruwan Kiringoda Sarah Hong
Colonoscopy Colonoscopy is the best technique for examination of the large intestine, and for the biopsy and treatment of mucosal lesions
Data Source for the Project The Cleveland Clinic in Cleveland, Ohio Conducted by a group member at the Cleveland Clinic, this study examined the frequency and impact of problems that interfere with smooth colonoscopy
Goals of the Study • To create an objective, quantifiable method of measuring the efficiency with which a doctor operates • To determine whether there are mathematically significant differences in efficiency levels between doctors • Determine what independent factors may be responsible for varying efficiency levels and to what degree each factor is responsible.
Background • Colonoscopy is the visual examination of the large intestine (colon) using a lighted, flexible fiber-optic or video endoscope.
Background (con’t) • The colon begins in the right-lower abdomen and looks like a big question mark as it moves through the abdomen, ending in the rectum. It is 5 to 6 feet long.
Equipment • The flexible colonoscope can be directed and moved around the many bends of the colon • The scope uses a small, optically-sensitive computer chip at the end.
Equipment (con’t) • Electronic signals are transmitted to the computer. • An open channel in the scope allows other instruments to be passed through in order to perform biopsies, remove polyps, etc.
Benefits • Identification and/or correction of a problem in the colon. • Allows for diagnosis and specific treatment.
The Study (some numbers to keep in mind) • Five staff surgeons were observed as they performed colonoscopies. • A total of 203 colonoscopies were observed. • The study began in June 2002 and concluded the following September. • 104 men, 99 women. • Mean age of 61; standard deviation of 12 years.
Efficiency Errors • The study focused on the incidence of potential efficiency problems that occur during the implementation of the procedure. • The phrase ‘efficiency error’ was used to define any error in setup, procedure or scope function that results in the avoidable loss of time. • The researcher quantified how much time was lost by using a stopwatch.
Four Types of Errors • Setup - valves, caps, hoses not fastened securely • Scope function - scope clogged • Procedural - Switching colonoscope midway through the exam, errors by trainees. • Torque - Scope hose overly twisted, needs to be re-set.
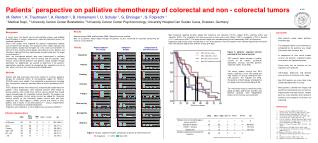
Statistical Analysis, Chi- Squared Test 1 Graph 1: Ho: p = .376 Ha: P .376 ChiTest([28.97,12.04,3.39,21.07,10.53 ],[41,32,9,56,28]); "The chi-squared value is", 134.2603333, "where there are", 5, "classes, and a probability of about ", 0., "percent that the null hypothesis is true and we see such chi squared value." "In particular this test is highly significant and we may reject the null hypothesis based on it"
Statistical Analysis, Chi- Squared Test 2 Graph 2: Ho: p = .280 Ha: P .280 ChiTest([8.96,2.52,15.68,7.84 ],[9,1,16,9]); "The chi-squared value is", 1.095167234, "where there are", 4, "classes, and a probability of about ", 77.82408589, "percent that the null hypothesis is true and we see such chi squared value.” "In particular this test is not significant and we should not reject the null hypothesis based on it"
Part II • What factors could potentially affect the colonoscopists’ incidence of error? • Possible factors: • Years of Practice at the Cleveland Clinic • Level of Specialty Education • Ex: Residencies, fellowships, graduate degrees • Number of American Board Certifications
Years Practicing Regression of Percentage Errors on = 0.05 with 3 d.f T = 2.77 Critical value = 2.353
Regression of Percentage Errors on Years of Specialty Education • = 0.05 with 3 d.f T = -2.24 • Critical value = 2.353
Regression of Percentage Errors on Number of Board Certifications = 0.05 with 3 d.f T = -3.90 Critical value = 2.353
Multivariate Regression of Percentage Errors on Years Practicing, Years of Specialty Education and Number of Board Certifications
Regression Analysis • All three variables appear to be negatively related to percentage of efficiency errors • Relation is not strong enough to be statistically conclusive • Directions of correlations “appear” right, but more doctors need to be sampled to obtain medical significance.
Conclusions • By a medically-acceptable level of significance, one of the doctors was found to be operating at a far inferior efficiency level than the other endoscopists. • “Efficiency errors,” however, refer only to small errors that result in a loss of time for the procedure. They do not, necessarily have an impact on patient safety or welfare.
Implications • If a doctor can be established in a court of law as being inferior, then potential litigation could be brought by unknowing patients who experience deleterious effects as a result of inferior treatment. • Patients should know of a doctor’s track record before undergoing the procedure
Limitations of this study • Number of trials • Only 202. • Perforated colons, the most serious of operational errors, only occur in 1/1000 operations. • Number of doctors • Only 5. • What would a study of 500 doctors yield?
Summary • The overall scope of the study is limited • Does not take into account other factors • Patient experience in terms of suffering • Risk • As outlined by the abstract, we have met the goals set forth in this presentation. Overall, this study provides a helpful and informative framework for future studies.