Download
1 / 32
330 likes | 519 Views
National Alopecia Areata Registry. Madeleine Duvic, MD Professor of Medicine & Dermatology MD Anderson Cancer Center Houston, Texas. Making the Diagnosis of AA. Characteristic patches of hairloss with broken off hairs - exclammation points

E N D
National Alopecia Areata Registry • Madeleine Duvic, MD • Professor of Medicine & Dermatology • MD Anderson Cancer Center • Houston, Texas
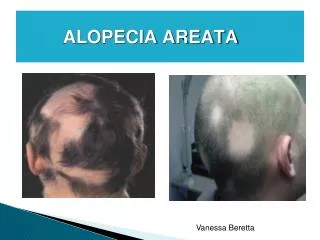
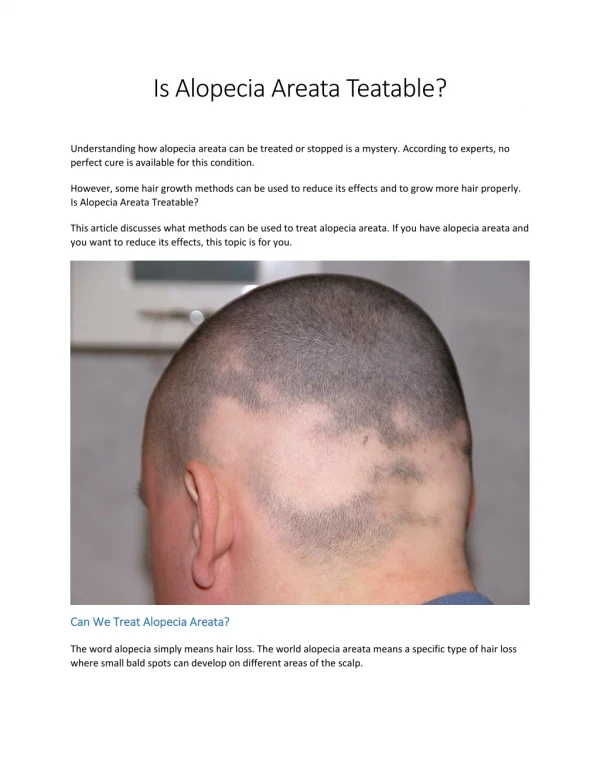
Making the Diagnosis of AA • Characteristic patches of hairloss with broken off hairs - exclammation points • Scale, redness may or may not be present. Biopsy is diagnostic. • Must rule out tinea capitus, lupus, MF, scarring alopecias, syphillis, etc. • Onset before 6 mos, suggests papular atricia with mutation in hairless gene chrom 8.
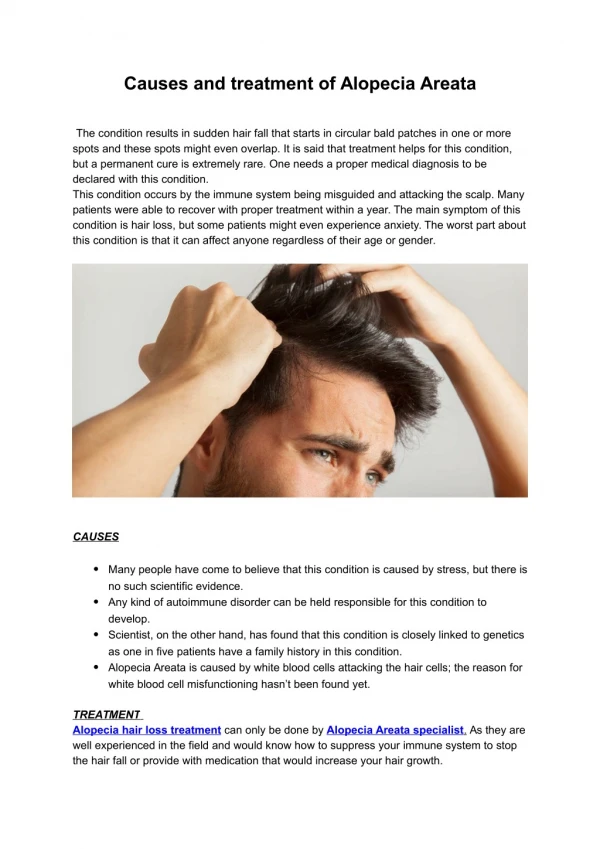
What causes AA? • Immune reaction by T-cells that are white blood cells called lymphocytes. • They surround hair follicles, causing breakage of growing hairs and bald spots. • What are they reacting to? Hair? Infection? • Virus? Melanocytes? unknown
HYPOTHESIS: Alopecia Areata is • Host determined • HLA restricted • Organ specific • Reaction directed to the hair follicle • Triggered by an external event, infection & • Mediated by cytokines & neuropeptides locally.
Is AA caused by genes? • T cells talk to messenger cells (interleukins) divide, and release of mediators (cytokines, chemokines) that start, intensify, and stop inflammation. • These mediators are turned on by genes and made by genes. • What the immune system reacts to is also caused by genes.
HLA - histocompatibility • Proteins that tell your cells that you are you are called HLA or histocompatibility antigens. • Must be matched in case of transplants • Bind to and show foreign proteins to T cells. • They control what gets seen by T cells
The Trimolecular Complex • T cells recognize Antigen when presented by HLA chains on APC Antigen Presenting Cell T cell Costimulatory CD4 or CD8 HLA Class 2 (CD4) T cell receptor
HF presents Antigen to T cells • CD4 T cells help B’s make Antibodies B CD4 APC HF Y Y Kerat Y Y Interferon Gamma HAIR Follicle Y
The Hair Follicle is Attacked ! • Cytotoxic CD8 T cells could initiate AA CD4 B APC CD8 HF Y Y Helper Kerat Y Interferon Gamma Cytotoxic Y HAIR Follicle Y
The Hair Follicle is Innocent ! • A Viral or other trigger initiates the CD8 or the CD4 Response - Molecular Mimicry CD4 APC CD8 Kerat HF Helper Interferon Gamma Y Cytotoxic Y HAIR Follicle Y
Class II HLA Associations • CLASS II MHC (DR,DQ,DP) ASSOCIATIONS • HLA-DR4, DR5 (Italian, Danish, & English); HLA-DR7 (Russians) • HLA-DR5 allele DR-1104-patchy early onset • 80% of AA have HLA-DQB1*03 alleles • Welsh/Duvic JID 103: 758,1994 • Colombe/Price JAAD 33:757, 1995
How many genes cause AA? • Not one!! Or else half of the children would inherit it • Not two!! One fourth of the children would inherit. • Multiple genes in autoimmune diseases: start it,keep it going, amplifiy, & stop it. • Often genes from both parents contribute. • Chances of having another offspring are small.
AA in Identical Twins • 55% concordancy in monozygotic twins. • More severe in first affected, M>>F. • All had HLA-DQ 0*302 • Stress was precipitating factor • No association with CMV • Jackow & Duvic, JAAD 1998.
Inheritance of AA • Identical twins – only half are both affected • Environmental trigger ??? • Or low penetrance • Hard to find families with more than three members affected with AA = multiplex family. These are ideal for studying the genes causing AA.
Purpose of the AA Registry • 1. To find and collect samples from multiplex families, siblings, and individuals with alopecia areata. • 2. To encourage research using the data and samples from the registry. • 3. By understanding AA to find effective treatments or cures.
Who Funds the Registry? • You do! Tax dollars • National Institutes of Health – Institute for Arthritis, Musculoskeletal, and Skin (NIAMS) • Competition for Registry contract • Awarded in 2001 to consortium of five centers to establish and maintain.
AlopeciaAreataRegistry.orgREGISTRATION on WEB or Print-out, Fill-out, & Mail or Fax in
Registration is Two Steps • Step One: General Registration of AA patients using short input form. (Web, Doctor or patient initiated) AlopeciaAreataRegistry.org • Step Two: patient must visit one of five sites or derm for exam, questionnaire, and sample collection.
Registration Sites • Minneapolis, Minn. – Maria Hordinsky • New York City – Columbia – Angela Christiano • Denver, Colorado – David Norris • Houston, Texas – Madeleine Duvic • San Francisco, Calif – Vera Price
Informed consent • Must have a signed consent to participate in step 2 of the registry. Document describing the research study. • Disclosure of pros and cons. • Place for patient and witness and doctor to sign if patient agrees to participate. Children can give their assess, parents their consent.
Who Can Register in First Tier? • United States Resident • Alopecia Areata – patchy loss Alopecia Totalis – all scalp hair Alopecia Universalis – scalp/body • Diagnosis is confirmed by a Dermatologist.
Progress Report Registration to date:4,984 3,380 women 1,604 men Race: Caucasians: 3901 African Am: 189 Asian: 189 Hispanic: 267
Breakdown of AA • Alopecia Universalis 1102 • Alopecia Totalis 462 • Patchy persistant AA 1040 • Transient AA 980 • Unconfirmed AA 50 • All AA 3122 • Controls 1369
After registering what next? • Information is completed by email or paper. • Patient invited for exam at center. • Signs consent and has brief exam • Donate blood for DNA, Cell lines, and serum banking. • Solicits family members and controls to help.
Selection of the Second Tier? • Multiplex Families – three or more affected persons with AA/AT/AU • Affected Sib-pairs/twins and parents
Selection for the Second Step • Single patients examined at site. • AT/AU for > 1 year • Patchy persistent AA for > 1 year • Transient AA for < 6 or < 12 mos. with complete regrowth • Unrelated Normal controls are just as important as AA subjects.
Optional Components • Collection of Biopsies by sites • Digital photography • Quality of Life questionnaires
Progress Report • Multiplex Families: 145 • Sib pairs: 54 • Simplex family 167 • Singles 559 • Unaffected controls 254 • Unrelated controls 271 • TOTAL 1,451
Type of AA in Registry • Persistent patchy AA 277 • Transient AA 209 • Alopecia Totalis (scalp) 104 • Alopecia Universalis 335 • Controls unrelated 271 • All AAs 925 • Goals: 500 of each
Progress in AA Research • Confirmed the HLA associations in Registry AA • Studies of cytokine profiles in AA with or without atopy. • Incidence of autoimmunity in AA • Quality of life in adolescents with AA • Linkage studies identified four regions where alopecia areata genes are present.
Enlisting Dermatology • Please tell every AA patient about the registry, distribute the brochures. • Take an AA family history - identify multiplex families/ sib-pairs. • Draw samples on multiplex families, sib-pairs who cannot travel to one of five sites.
Goals for this conference • To help anyone who wants to register do it. • To get all families with 3 or more AA cases, all twins, all sib pairs for linkage studies. • To go above 5000 registrations today • To go above 1000 AA second step registrations this meeting. • To answer your questions!!!