Download
1 / 29
310 likes | 879 Views
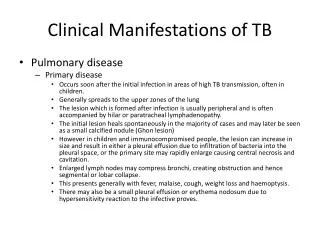
Pulmonary Manifestations of SLE. Ted Carter, MD Atlanta Medical Center. Pulmonary Manifestations of SLE. Pleuritic Chest Pain Upper Respiratory Tract Infections Acute Pneumonitis Chronic Pneumonitis Pulmonary Hypertension Shrinking Lung Syndrome Pulmonary Hemorrhage Other.

E N D
Pulmonary Manifestations of SLE Ted Carter, MD Atlanta Medical Center
Pulmonary Manifestations of SLE • Pleuritic Chest Pain • Upper Respiratory Tract Infections • Acute Pneumonitis • Chronic Pneumonitis • Pulmonary Hypertension • Shrinking Lung Syndrome • Pulmonary Hemorrhage • Other
Pleuritic Chest Pain • Musculoskeletal pain • Pleuritis
Pleuritic Chest PainMusculoskeletal • 50% of SLE patients experience musculoskeletal or pleuritic chest pain • Most commonly from muscle, connective tissue, or costochondral joints (Tietze’s syndrome) • Responds to local heat, NSAIDs, topical analgesics, and Tylenol
Pleuritic Chest PainPleuritis • Difficult to diagnose • Rub and/or pleural effusion (20%) may be present • Effusion is usually small or moderate • Effusion is a mild exudate with elevated LDH, but no signs of marked inflammation
Pleuritic Chest PainEffusions • Generally, • Total white cell count is lower in SLE • Glucose levels are slightly lower than plasma levels in SLE • Low complement levels • Protein concentration is low in SLE
Pleuritic Chest PainEffusions • Don’t forget to exclude: • Infection • CHF • Uremia
Upper Respiratory Tract Infection • Usually presents as a cough • Usually viral • More frequent in SLE patients due to treatment with corticosteroids or immunosuppressive drugs
Pneumonitis • Acute • Chronic
Acute PneumonitisClinical • Uncommon, 1-12% • Fever, cough, hemoptysis, pleurisy, dyspnea • Hypoxia, basilar rales • Pleural effusion (50%) • Pulmonary infiltrates, usually lower lobes • No pathogen can be isolated
Acute PneumonitisPathology • Acute alveolar wall injury • Alveolar hemorrhage • Alveolar edema • Hyaline membrane formation • Immunoglobulin and complement deposition • Some authors require one of the following for diagnosis: interstitial fibrosis, vasculitis, hematoxylin bodies, interstitial pneumonitis, alveolitis, or pleuritis
Acute PneumonitisPrognosis and Treatment • Prognosis is generally poor • Short term mortality of 50%! • If developed during postpartum period, prognosis is very poor • Survivors have persistent PFT abnormalities with restrictive defects • Give antibiotics pending culture results • Prednisone is mainstay…1.5mg/kg qd
Chronic PneumonitisClinical • Up to 9% of patients with SLE • Frequently preceded by acute pneumonitis • Longstanding SLE more likely • Anti-Ro antibodies more likely • Chronic non-productive cough, dyspnea, and recurrent pleuritic chest pain • PFTs show restrictive pattern with decreased lung volume • ABGs show decreased Dlco and pO2
Chronic PneumonitisDiagnosis • Differentiate from Pulmonary edema ARDS Bilateral pneumonia Interstitial fibrosis Infection Malignancy Granulomatous disease
Chronic PneumonitisDiagnosis • HRCT useful • Look for • ground glass appearance, or • reticular pattern
Chronic PneumonitisDiagnosis • HRCT useful • Look for ground glass appearance, or • reticular pattern • Bronchioalveolar lavage (BAL)
Chronic PneumonitisDiagnosis using Bronchioalveolar Lavage • Use to exclude infection, malignancy, and granulomatous disease • >10% neutrophils suggests Chronic Pneumonitis • This finding is also observed in: Scleroderma Rheumotoid pneumonitis Idiopathic pulmonary fibrosis • Lupus is suggested by characteristic serological and extrapulmonary findings
Chronic PneumonitisTreatment • Oral prednisone at 1mg/kg qday • Expect slow improvement or stabilization • Immunosuppressive agents if no response
Pulmonary Hypertension • Rare complication of SLE • Symptoms range from dyspnea, chronic non-productive cough and chest pain to… • Fatigue, weakness, palpitations, edema, ascites and RVH • Diagnosis by echocardiogram, or right sided cardiac catheterization
Pulmonary Hypertension • Treatment includes oxygen, anticoagulants and vasodilators (Calcium blockers and prostacyclin infusion) • Poor prognosis with one study showing 50% 5-year mortality
Shrinking Lung Syndrome • Characterized by dyspnea, pleuritic chest pain, and progressive decrease in lung volume • Chest X-RAY is clear, with elevated diaphragms • Mechanism is unclear • Treatment with corticosteroids
Pulmonary Hemorrhage • Not necessarily associated with hemoptysis • Presenting manifestation of SLE in 10-20% of cases • CXR shows bilateral alveolar infiltrates • Unknown etiology • Bleeding can induce anemia
Pulmonary Hemorrhage • Diagnosis by lung biopsy • Treat with high dose corticosteroids, cyclophosphamide, and aggressive support • Plasmapheresis for patients who fail steroids • Survival ranges from 50-70%
Other Pulmonary Disorders • Bronchiolitis obliterans with organizing pneumonia (BOOP) • Prednisone 1mg/kg qday, or • cyclophosphamide • Acute reversible hypoxemia • Elevated C3a • Pulmonary leukoaggregation and complement activation • Corticosteroids and aspirin
Other Pulmonary Disorders • ARDS • Commonly due to bacteremia with Gm- bacteria • More likely in those treated with steroids within the previous month • 68% mortality
Other Pulmonary Disorders • Antiphospholipid antibodies • Pulmonary embolism • Thromboembolic and nonthromboembolic pulmonary hypertension • Pulmonary artery thrombosis • ARDS • Postpartum HUS • Treat with chronic anticoagulation