Download

1 / 33
340 likes | 372 Views
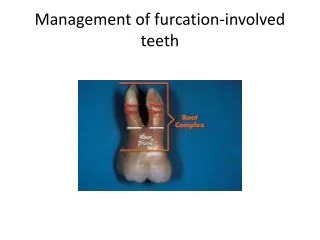
Artificial Floor Concept for the Repair of Furcation Perforation. Hatem A. Alhadaiy. Background. Artificial opening occurs in the pulp wall creating communication between the pulp and the exterior. Root Perforation.

E N D
Artificial Floor Concept for the Repair of Furcation Perforation Hatem A. Alhadaiy
Background Artificial opening occurs in the pulp wall creating communication between the pulp and the exterior. Root Perforation
Traumatic (iatrogenic) perforations are due to lack of attention given to details of dental anatomy and failure to consider its variations by the clinician. Traumatic Perforations
Causes • Usually occur due to inattentive access opening. • Perforation of a pulp chamber floor may result if the bur is not properly angulated in relation to the long axis of the tooth.
How to avoid traumatic perforations • A thorough knowledge of the internal anatomy and the possible anatomical variations of root canal system. • Proper case selection and treatment planning
Obtaining adequate straight access to the root canal with total removal of the pulp chamber roof. • When a root-filling material is removed during post preparation, the canal should be periodically cleaned and examined to ensure that the cutting action of the bur end is confined to the root canal space.
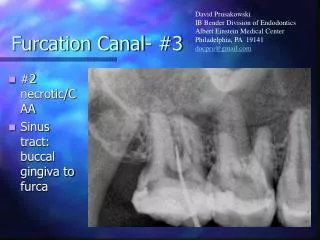
Diagnosis • Direct observation (magnification) b) Paper points c) Radiographs d) Electronic apex locators e) Symptomatic findings
Existing perforation • The presence of serous exudate in the site of the perforation • Sensitivity of the involved tooth to percussion Chronic inflammation of the gingiva • The presence of a sinus tract or the appearance of localized problems such as pocket formation or furcation involvement following an apparently adequate endodontic therapy may indicate the existence of perforation.
Factors affecting prognosis 1) Time lapsed before obturating the defect 2) Location of the perforation 3) Size of the perforation 4) Adequacy of the perforation seal 5) Repair material.
Surgicalrepair • Reflecting a flap at the perforation site and packing a repair material into the defect. • Preparing the perforation site using ultrasonic handpiece with the aid of surgical microscope.
Bicuspidization is a process of molar tooth sectioning and maintaining of both sections followed by their crowning to serve as two premolars. • Root amputation is a process of removal of the defected root after molar sectioning, keeping the sound root intact. • Surgical-nonsurgical approach
Nonsurgical repair • Surgical approach often leads to loss of attachment, chronic pocket formation, and periodontal furcation involvement. • Furcation perforations are usually less accessible for surgical approach especially if the perforation is lingually situated, or if it is located in the furcation area of a maxillary molar. • Perforations coronal to gingival attachment may be conventionally repaired with a restorative material or a crown.
Different materials have been used for nonsurgical repair of perforation defects • amalgam, • gutta percha, • calcium hydroxide, • Cavit (Premier dental produclx. Philadelphia). • MTA • Others
Repair material extrusion into the periodontal space using bioinert matrices: • indium foil matrices • Dentin chips and calcium hydroxide • Perforations to be filled with blood and obturated the orifices with either calcium hydroxide or Teflon discs. • Hhydroxyapatite or tricalcium phosphate matrix. • MTA (Mineral trioxide aggregate) used without internal matrix.
Objectives The objectives of repairing furcation perforations are to seal the dentin defect and provide suitable conditions for formation of a new periodontal attachment.
Some materials may provide adequate seal but may interfere with the formation of periodontal reattachment due to their extrusion into the furcation area. • Periodontal reattachment did not occur when materials like amalgam, gutta percha, or calcium hydroxide were used for perforation repairs.
Materials such as hydroxyapatite or plaster of Paris may initiate formation of new bone and periodontal attachment but can not adequately seal the dentin defect. This may result in leakage of bacteria and then by-products into the lesion and failure, especially the perforation is connected to the oral cavity.
Since the furcation perforation involves differenl types of inter-related tissues, each tissue within the defect should be considered separately. • Alhadainy et al. suggested the use of artificial floor technique for repairing furcation perforations considering the periodontal wound and the dentinal wound as separate identities.
Artificial Floor Technique Artificial floor versus internal matrix
Perforation Periodontal ligament Bone
Gutta percha Perforation Periodontal ligament Bone
Gutta percha Perforation Artificial floor Periodontal ligament Bone
Gutta percha Perforation Artificial floor Periodontal ligament Bone
Gutta percha Repair material Artificial floor Periodontal ligament Bone
Repair material Artificial floor Periodontal ligament Bone
Composite resin Repair material Artificial floor Gutta percha Periodontal ligament Bone
Calcium sulfate (plaster of Paris ) was used under glass ionomer to repair furcation perforations. plaster of Paris is stable, biocompatible, readily available, easily sterilizable, and shows rapid rate of resorption coinciding with the rate of new bone growth. It also accelerates the rate of mineralization of the new bone by providing a ready source of calcium ions for early mineralization process.Calcium sulfate acts as bone barrier, aids guided bone regeneration and excludes epithelial tissue from the site of bone formation. This may help in avoiding the formation of periodontal pockets and allows for periodontal reattachment.